
Taxiway Overflight
Air Canada Flight 759
Airbus A320-211, C-FKCK
San Francisco, California
July 7, 2017
Incident Report
NTSB/AIR-18/01
PB2018-101561
National
Transportation
Safety Board
NTSB/AIR-18/01
PB2018-101561
Notation 58387
Adopted September 25, 2018
Aircraft Incident Report
Taxiway Overflight
Air Canada Flight 759
Airbus A320-211, C-FKCK
San Francisco, California
July 7, 2017
National
Transportation
Safety Board
490 L’Enfant Plaza, S.W.
Washington, DC 20594
National Transportation Safety Board. 2018. Taxiway Overflight, Air Canada Flight 759, Airbus
A320-211, C-FKCK, San Francisco, California, July 7, 2017. NTSB/AIR-18/01. Washington, DC.
Abstract: This report discusses the July 7, 2017, incident involving Air Canada flight 759, an Airbus
A320-211, Canadian registration C-FKCK, which was cleared to land on runway 28R at San Francisco
International Airport, San Francisco, California, but instead lined up with parallel taxiway C. Four air
carrier airplanes were on taxiway C awaiting clearance to take off from runway 28R. The incident airplane
descended to an altitude of 100 ft above ground level and overflew the first airplane on the taxiway. The
incident flight crew initiated a go-around, and the airplane reached a minimum altitude of about 60 ft and
overflew the second airplane on the taxiway before starting to climb. None of the 5 flight crewmembers
and 135 passengers aboard the incident airplane were injured, and the incident airplane was not damaged.
Safety issues identified in this report include the need for consistent flight management system autotuning
capability within an air carrier’s fleet, the need for more effective presentation of flight operations
information to optimize pilot review and retention of relevant information, the need for airplanes landing
at primary airports within Class B and Class C airspace to be equipped with a system that alerts pilots when
an airplane is not aligned with a runway surface, the need for modifications to airport surface detection
equipment systems to detect potential taxiway landings and provide alerts to air traffic controllers, the need
for a method to more effectively signal a runway closure to pilots when at least one parallel runway remains
in use, and the need for revisions to Canadian regulations to address the potential for fatigue for pilots on
reserve duty who are called to operate evening flights that would extend into the pilots’ window of circadian
low. As a result of this investigation, the National Transportation Safety Board makes safety
recommendations to the Federal Aviation Administration and Transport Canada.
The National Transportation Safety Board (NTSB) is an independent federal agency dedicated to promoting aviation,
railroad, highway, marine, and pipeline safety. Established in 1967, the agency is mandated by Congress through the
Independent Safety Board Act of 1974 to investigate transportation accidents, determine the probable causes of the
accidents, issue safety recommendations, study transportation safety issues, and evaluate the safety effectiveness of
government agencies involved in transportation. The NTSB makes public its actions and decisions through accident
reports, safety studies, special investigation reports, safety recommendations, and statistical reviews.
The NTSB does not assign fault or blame for an accident or incident; rather, as specified by NTSB regulation,
“accident/incident investigations are fact-finding proceedings with no formal issues and no adverse parties … and are
not conducted for the purpose of determining the rights or liabilities of any person.” 49 C.F.R. § 831.4. Assignment
of fault or legal liability is not relevant to the NTSB’s statutory mission to improve transportation safety by
investigating accidents and incidents and issuing safety recommendations. In addition, statutory language prohibits
the admission into evidence or use of any part of an NTSB report related to an accident in a civil action for damages
resulting from a matter mentioned in the report. 49 U.S.C. § 1154(b).
For more detailed background information on this report, visit
https://www.ntsb.gov/investigations/SitePages/dms.aspx and search for NTSB incident ID DCA17IA148. Recent
publications are available in their entirety on the Internet at http://www.ntsb.gov. Other information about available
publications also may be obtained from the website or by contacting:
National Transportation Safety Board
Records Management Division, CIO-40
490 L’Enfant Plaza, SW
Washington, DC 20594
(800) 877-6799 or (202) 314-6551
Copies of NTSB publications may be downloaded at no cost from the National Technical Information Service’s
National Technical Reports Library at https://ntrl.ntis.gov/NTRL/ (this product is product number PB2018-101561).
For additional assistance, contact:
National Technical Information Service (http://www.ntis.gov/)
5301 Shawnee Rd.
Alexandria, VA 22312
(800) 553-6847 or (703) 605-6000
NTSB Aircraft Incident Report
i
Contents
Figures ........................................................................................................................................... iii
Tables ............................................................................................................................................ iv
Abbreviations .................................................................................................................................v
Executive Summary ................................................................................................................... viii
1. Factual Information ...................................................................................................................1
1.1 History of Flight .........................................................................................................................1
1.1.1 Preceding Arrival on Runway 28R ..................................................................................9
1.1.2 Airplanes on Taxiway C ................................................................................................10
1.2 Personnel Information ..............................................................................................................10
1.2.1 The Captain ....................................................................................................................10
1.2.2 The First Officer ............................................................................................................12
1.3 Airplane Information ...............................................................................................................13
1.4 Airport Information ..................................................................................................................14
1.4.1 Air Traffic Control Tower Staffing ...............................................................................18
1.4.2 Air Traffic Control Tower Equipment ...........................................................................20
1.5 Tests and Research ...................................................................................................................22
1.5.1 Airplane Performance Study ..........................................................................................22
1.5.2 Enhanced Ground Proximity Warning System Simulation ...........................................25
1.6 Organizational Information ......................................................................................................26
1.6.1 Descent, Approach, and Arrival Information ................................................................26
1.6.2 Crew Resource Management .........................................................................................28
1.6.3 Fatigue Information .......................................................................................................29
1.6.4 Event Reports .................................................................................................................29
1.6.5 Plan Continuation and Expectation Bias Training .........................................................31
1.6.6 Flight Information ..........................................................................................................32
1.7 Additional Information ............................................................................................................36
1.7.1 Wrong Surface Landings Video ....................................................................................36
1.7.2 Safety Alert for Operators .............................................................................................36
1.7.3 Canadian Fatigue Regulations .......................................................................................37
2. Analysis .....................................................................................................................................39
2.1 Introduction ..............................................................................................................................39
2.2 Incident Sequence ....................................................................................................................40
2.2.1 Notification of Runway 28L Status ...............................................................................40
2.2.2 Preparations for the Descent ..........................................................................................40
2.2.3 Initial Approach .............................................................................................................42
2.2.4 Final Approach Segment and Go-Around .....................................................................43
2.2.5 Crew Resource Management Breakdown .....................................................................45
2.3 Reasons for Flight Crew’s Misalignment With Taxiway C.....................................................47
NTSB Aircraft Incident Report
ii
2.3.1 Flight Crew Awareness of Runway Closure .................................................................47
2.3.2 Role of Expectation Bias ...............................................................................................49
2.3.2.1 Initial Taxiway Misalignment ..........................................................................49
2.3.2.2 Flight Crew Recognition of Misalignment ......................................................51
2.3.3 Role of Flight Crew Fatigue ..........................................................................................52
2.3.4 Mitigations to Overcome Expectation Bias ...................................................................55
2.4 Reporting of the Incident Flight ...............................................................................................58
2.5 Air Traffic Control Services ....................................................................................................59
2.5.1 Air Traffic Control Tower Midnight Shift Staffing .......................................................59
2.5.2 Airport Surface Surveillance Capability System ...........................................................61
2.6 Runway Closure Markers ........................................................................................................63
3. Conclusions ...............................................................................................................................66
3.1 Findings....................................................................................................................................66
3.2 Probable Cause.........................................................................................................................68
4. Recommendations ....................................................................................................................69
Board Member Statements .........................................................................................................71
5. Appendixes ...............................................................................................................................76
Appendix A: Investigation .............................................................................................................76
Appendix B: Air Canada Postincident Actions .............................................................................77
References .....................................................................................................................................78
NTSB Aircraft Incident Report
iii
Figures
Figure 1. ACA759 track over SFO. ................................................................................................6
Figure 2. Incident airplane. ...........................................................................................................14
Figure 3. SFO layout map. ............................................................................................................15
Figure 4. Illustration of SFO’s lighting configuration. .................................................................16
Figure 5. ASSC display at SFO. ...................................................................................................21
Figure 6. ACA759 on final approach to SFO. ..............................................................................23
Figure 7. ACA759 passing over UAL1 and relative locations of airplanes. ................................24
Figure 8. ACA759 passing over PAL115 and relative locations of airplanes. .............................24
Figure 9. Approach procedure. .....................................................................................................34
Figure 10. NOTAM showing runway 28L closure. ......................................................................35
Figure 11. ATIS information Quebec. ..........................................................................................36
NTSB Aircraft Incident Report
iv
Tables
Table 1. Timeline of events. ............................................................................................................8
Table 2. Captain’s self-reported sleep schedule. ...........................................................................12
Table 3. First officer’s self-reported sleep schedule. ....................................................................13
NTSB Aircraft Incident Report
v
Abbreviations
AC advisory circular
ACA759 Air Canada flight 759
ACARS aircraft communication addressing and reporting system
agl above ground level
ASDE airport surface detection equipment
ASR air safety report
ASRS aviation safety reporting system
ASSC airport surface surveillance capability
ATC air traffic control
ATCT air traffic control tower
ATIS automatic terminal information service
CAST Commercial Aviation Safety Team
CFR Code of Federal Regulations
CRM crew resource management
CVR cockpit voice recorder
DAL521 Delta Air Lines flight 521
EDT eastern daylight time
EGPWS enhanced ground proximity warning systems
FAA Federal Aviation Administration
FDR flight data recorder
NTSB Aircraft Incident Report
vi
FMC flight management computer
FMGS flight management guidance system
FMS flight management system
IFR instrument flight rules
ILS instrument landing system
LNAV lateral navigation
LUAW line up and wait
MCDU multifunction control and display unit
msl mean sea level
NCT Northern California terminal radar approach control
nm nautical mile
NOTAM notice to airmen
NTSB National Transportation Safety Board
PAL115 Philippine Airlines flight 115
PDT Pacific daylight time
PFD primary flight display
RAAS runway awareness and advisory system
RNAV area navigation
SAFO safety alert for operators
SEA Seattle-Tacoma International Airport
SFO San Francisco International Airport
NTSB Aircraft Incident Report
vii
TSB Transportation Safety Board of Canada
UAL1 United Airlines flight 1
UAL863 United Airlines flight 863
UAL1118 United Airlines flight 1118
VMC visual meteorological conditions
YYZ Toronto/Lester B. Pearson International Airport

NTSB Aircraft Incident Report
viii
Executive Summary
On July 7, 2017, about 2356 Pacific daylight time (PDT), Air Canada flight 759, an
Airbus A320-211, Canadian registration C-FKCK, was cleared to land on runway 28R at
San Francisco International Airport (SFO), San Francisco, California, but instead lined up with
parallel taxiway C.
1
Four air carrier airplanes (a Boeing 787, an Airbus A340, another Boeing 787,
and a Boeing 737) were on taxiway C awaiting clearance to take off from runway 28R. The
incident airplane descended to an altitude of 100 ft above ground level and overflew the first
airplane on the taxiway. The incident flight crew initiated a go-around, and the airplane reached a
minimum altitude of about 60 ft and overflew the second airplane on the taxiway before starting
to climb. None of the 5 flight crewmembers and 135 passengers aboard the incident airplane were
injured, and the incident airplane was not damaged.
2
The incident flight was operated by
Air Canada under Title 14 Code of Federal Regulations (CFR) Part 129 as an international
scheduled passenger flight from Toronto/Lester B. Pearson International Airport, Toronto,
Canada. An instrument flight rules flight plan had been filed. Night visual meteorological
conditions prevailed at the time of the incident.
The flight crewmembers had recent experience flying into SFO at night and were likely
expecting SFO to be in its usual configuration; however, on the night of the incident, SFO parallel
runway 28L was scheduled to be closed at 2300. The flight crew had opportunities before
beginning the approach to learn about the runway 28L closure. The first opportunity occurred
before the flight when the crewmembers received the flight release, which included a notice to
airmen (NOTAM) about the runway 28L closure. However, the first officer stated that he could
not recall reviewing the specific NOTAM that addressed the runway closure. The captain stated
that he saw the runway closure information, but his actions (as the pilot flying) in aligning the
airplane with taxiway C instead of runway 28R demonstrated that he did not recall that information
when it was needed. The second opportunity occurred in flight when the crewmembers reviewed
automatic terminal information system (ATIS) information Quebec (via the airplane’s aircraft
communication addressing and reporting system [ACARS]), which also included NOTAM
information about the runway 28L closure. Both crewmembers recalled reviewing ATIS
information Quebec but could not recall reviewing the specific NOTAM that described the runway
closure.
The procedures for the approach to runway 28R required the first officer (as the pilot
monitoring) to manually tune the instrument landing system (ILS) frequency for runway 28R,
which would provide backup lateral guidance (via the localizer) during the approach to supplement
the visual approach procedures. However, when the first officer set up the approach, he missed the
step to manually tune the ILS frequency. The captain was required to review and verify all
programming by the first officer but did not notice that the ILS frequency had not been entered.
The captain stated that, as the airplane approached the airport, he thought that he saw
runway lights for runway 28L and thus believed that runway 28R was runway 28L and that
1
All times in this executive summary are PDT unless otherwise noted.
2
Similarly, no crewmembers and passengers aboard the airplanes on taxiway C were injured, and none of those
airplanes were damaged.
NTSB Aircraft Incident Report
ix
taxiway C was runway 28R. At that time, the first officer was focusing inside the cockpit because
he was programming the missed approach altitude and heading (in case a missed approach was
necessary) and was setting (per the captain’s instruction) the runway heading, which reduced his
opportunity to effectively monitor the approach. The captain asked the first officer to contact the
controller to confirm that the runway was clear, at which time the first officer looked up. By that
point, the airplane was lined up with taxiway C, but the first officer presumed that the airplane was
aligned with runway 28R due, in part, to his expectation that the captain would align the airplane
with the intended landing runway.
The controller confirmed that runway 28R was clear, but the flight crewmembers were
unable to reconcile their confusion about the perceived lights on the runway (which were lights
from airplanes on taxiway C) with the controller’s assurance that the runway was clear. Neither
flight crewmember recognized that the airplane was not aligned with the intended landing runway
until the airplane was over the airport surface, at which time the flight crew initiated a low-altitude
go-around. According to the captain, the first officer called for a go-around at the same time as the
captain initiated the maneuver, thereby preventing a collision between the incident airplane and
one or more airplanes on the taxiway. However, at that point, safety margins were severely reduced
given the incident airplane’s proximity to the ground before the airplane began climbing and the
minimal distance between the incident airplane and the airplanes on taxiway C.
The flight crewmembers stated, during postincident interviews, that the taxiway C surface
resembled a runway. Although multiple cues were available to the flight crew to distinguish
runway 28R from taxiway C (such as the green centerline lights and flashing yellow guard lights
on the taxiway), sufficient cues also existed to confirm the crew’s expectation that the airplane
was aligned with the intended landing runway (such as the general outline of airplane lights—in a
straight line—on taxiway C and the presence of runway and approach lights on runway 28R, which
would also have been present on runway 28L when open). As a result, once the airplane was
aligned with what the flight crewmembers thought was the correct landing surface, they were likely
not strongly considering contradictory information. The cues available to the flight crew to indicate
that the airplane was aligned with a taxiway did not overcome the crew’s belief, as a result of
expectation bias, that the taxiway was the intended landing runway.
The flight crewmembers reported that they started to feel tired just after they navigated
through an area of thunderstorms, which radar data indicated was about 2145 (0045 eastern
daylight time [EDT]). The incident occurred about 2356, which was 0256 EDT according to the
flight crew’s normal body clock time; thus, part of the incident flight occurred during a time when
the flight crew would normally have been asleep (according to postincident interviews) and at a
time that approximates the start of the human circadian low period described in Air Canada’s
fatigue information (in this case, 0300 to 0500 EDT). In addition, at the time of the incident, the
captain had been awake for more than 19 hours, and the first officer had been awake for more than
12 hours. Thus, the captain and the first officer were fatigued during the incident flight.
Cockpit voice recorder (CVR) information was not available for this incident because the
data were overwritten before senior Air Canada officials became aware of the severity of this
incident. Although the National Transportation Safety Board (NTSB) identified significant safety
issues during our investigation into this incident, CVR information, if it had been available, could
have provided direct evidence about the events leading to the overflight and the go-around. For
NTSB Aircraft Incident Report
x
example, several crew actions/inactions during the incident flight demonstrated breakdowns in
crew resource management (CRM), including both pilots’ failure to assimilate the runway 28L
closure information included in the ATIS information, the first officer’s failure to manually tune
the ILS frequency, and the captain’s failure to verify the tuning of the ILS frequency. However,
without CVR information, the NTSB could not determine whether distraction, workload, and/or
other factors contributed to these failures.
The NTSB identified the following safety issues as a result of this incident investigation:
• Need for consistent flight management system (FMS) autotuning capability within an
air carrier’s fleet. The FMS Bridge visual approach to runway 28R was the only approach
in Air Canada’s Airbus A320 database that required manual tuning for a navigational aid,
so the manual tuning of the ILS frequency was not a usual procedure for the flight crew.
Identifying other approaches that require an unusual or abnormal manual frequency input
and developing an autotune solution would help preclude such a situation from recurring.
Further, the instruction on the approach chart to manually tune the ILS frequency was not
conspicuous during the crew’s review of the chart. An action to mitigate this situation for
other approaches would be to ensure sufficient salience of the manual tune entry on
approach charts.
• Need for more effective presentation of flight operations information to optimize pilot
review and retention of relevant information. The way information is presented can
significantly affect how information is reviewed and retained because a pilot could miss
more relevant information when it is presented with information that is less relevant.
Although the NOTAM about the runway 28L closure appeared in the flight release and the
ACARS message that were provided to the flight crew, the presentation of that information
did not effectively convey the importance of the runway closure information and promote
flight crew review and retention. Multiple events in the National Aeronautics and Space
Administration’s aviation safety reporting system database showed that this issue has
affected other pilots, indicating that all pilots could benefit from the improved display of
flight operations information.
• Need for airplanes landing at primary airports within Class B and Class C airspace
to be equipped with a system that alerts pilots when an airplane is not aligned with a
runway surface. A cockpit system that provides an alert if the system predicts a landing
on a surface other than a runway would provide pilots with additional positional awareness
information. Although the Federal Aviation Administration (FAA) has not mandated the
installation of such a system, the results of a simulation showed that such technology, if it
had been installed on the incident airplane, could have helped the flight crew identify its
surface misalignment error earlier in the landing sequence, which could have resulted in
the go-around being performed at a safer altitude (before the airplane was dangerously
close to other airplanes). Flight safety would be enhanced if airplanes landing at primary
airports within Class B and Class C airspace were equipped with such a cockpit system
and/or a cockpit system that alerts when an airplane is not aligned with the specific runway
for which it has been cleared.

NTSB Aircraft Incident Report
xi
• Need for modifications to airport surface detection equipment (ASDE) systems
(ASDE-3, ASDE-X, and airport surface surveillance capability [ASSC]) to detect
potential taxiway landings and provide alerts to air traffic controllers. The SFO air
traffic control tower was equipped with an ASSC system, which was not designed to
predict an imminent collision involving an arriving airplane lined up with a taxiway; thus,
the ASSC system did not produce an alarm as the incident airplane approached taxiway C.
If an airplane were to align with a taxiway, an automated ASDE alert could assist
controllers in identifying and preventing a potential taxiway landing as well as a potential
collision with aircraft, vehicles, or objects that are positioned along taxiways. An FAA
demonstration in February 2018 showed the potential effectiveness of such a system.
3
• Need for a method to more effectively signal a runway closure to pilots when at least
one parallel runway remains in use. A runway closure marker with a lighted flashing
white “X” appeared at the approach and departure ends of runway 28L when it was closed.
The runway closure marker was not designed to capture the attention of a flight crew on
approach to a different runway, and the marker did not capture the attention of the incident
flight crew as the airplane approached the airport while aligned with taxiway C. Increased
conspicuity of runway closure markers, especially those used in parallel runway
configurations, could help prevent runway misidentification by flight crews while on
approach to an airport.
• Need for revisions to Canadian regulations to address the potential for fatigue for
pilots on reserve duty who are called to operate evening flights that would extend into
the pilots’ window of circadian low. The flight crew’s work schedule for the incident
flight complied with the applicable Canadian flight time limitations and rest requirements;
however, the flight and duty time and rest requirements for the captain (a company reserve
pilot) would not have complied with US flight time limitations and rest requirements
(14 CFR Part 117). Transport Canada indicated that its current flight and duty time
regulations have been in effect since 1996. Transport Canada also indicated that it released
a draft of proposed new flight and duty time regulations in 2014 and issued revised draft
regulations in 2017. According to Transport Canada, the proposed regulations would better
address the challenge of fatigue mitigation for pilots on reserve duty who are called to
operate evening flights extending into their window of circadian low. However,
Transport Canada has not yet finalized its rulemaking in this area.
4
3
On March 2, 2011, the NTSB recommended that the FAA “perform a technical review of Airport Surface
Detection Equipment—Model X to determine if the capability exists systemwide to detect improper operations such
as landings on taxiways” (A-11-12). The NTSB also recommended that the FAA, “at those installation sites where the
technical review recommended in Safety Recommendation A-11-12 determines it is feasible, implement modifications
to Airport Surface Detection Equipment—Model X to detect improper operations, such as landings on taxiways, and
provide alerts to air traffic controllers that these potential collision risks exist” (A-11-13). As discussed in section
2.5.2, the NTSB classified these recommendations “Closed—Unacceptable Action” on September 14, 2011.
4
Title 14 CFR Part 117, “Flight and Duty Limitations and Rest Requirements: Flightcrew Members,” described
the window of circadian low as 0200 through 0559 (body clock time zone).
NTSB Aircraft Incident Report
xii
The NTSB determines that the probable cause of this incident was the flight crew’s
misidentification of taxiway C as the intended landing runway, which resulted from the
crewmembers’ lack of awareness of the parallel runway closure due to their ineffective review of
NOTAM information before the flight and during the approach briefing. Contributing to the
incident were (1) the flight crew’s failure to tune the ILS frequency for backup lateral guidance,
expectation bias, fatigue due to circadian disruption and length of continued wakefulness, and
breakdowns in CRM and (2) Air Canada’s ineffective presentation of approach procedure and
NOTAM information.
As a result of this investigation, the NTSB makes safety recommendations to the FAA and
Transport Canada.

NTSB Aircraft Incident Report
1
1. Factual Information
1.1 History of Flight
On July 7, 2017, about 2356 Pacific daylight time (PDT), Air Canada flight 759 (ACA759),
an Airbus A320-211, Canadian registration C-FKCK, was cleared to land on runway 28R at
San Francisco International Airport (SFO), San Francisco, California, but instead lined up with
parallel taxiway C.
1
Four air carrier airplanes (a Boeing 787, an Airbus A340, another Boeing 787,
and a Boeing 737) were on taxiway C awaiting clearance to take off from runway 28R. The
incident airplane descended to an altitude of 100 ft above ground level (agl) and overflew the first
airplane on the taxiway.
2
The incident flight crew initiated a go-around, and the airplane reached
a minimum altitude of about 60 ft and overflew the second airplane on the taxiway before starting
to climb. None of the 5 flight crewmembers and 135 passengers aboard the incident airplane were
injured, and the incident airplane was not damaged.
3
The incident flight was operated by
Air Canada under Title 14 Code of Federal Regulations (CFR) Part 129 as an international
scheduled passenger flight from Toronto/Lester B. Pearson International Airport (YYZ),
Toronto, Canada. An instrument flight rules (IFR) flight plan had been filed. Night visual
meteorological conditions (VMC) prevailed at the time of the incident.
4
The captain and the first officer reported for duty about 1640 and 1610 (1940 and 1910
eastern daylight time [EDT]), respectively. They met at the gate and discussed that the flight’s
departure would be delayed because the airplane to be used for the flight would be arriving at YYZ
late (due to weather in the Toronto area).
5
They also discussed the expected weather en route and
reviewed the flight release (also referred to as a dispatch release), which contained pertinent
information for the flight, including notice to airmen (NOTAM) information for SFO.
One of the NOTAMs in the dispatch release indicated that runway 28L would be closed
from 2300 that night to 0800 the next morning. During postincident interviews, both flight
crewmembers provided different accounts regarding their awareness of the runway closure.
6
During interviews about 1 week after the incident, the captain stated that he saw the NOTAM
about the runway 28L closure in the flight release, and the first officer stated that he did a “quick
1
(a) All times in this report are PDT unless otherwise noted. (b) This report also refers to ACA759 as the incident
airplane and the incident flight. (c) Title 49 Code of Federal Regulations 830.2 defined an incident as “an occurrence
other than an accident, associated with the operation of an aircraft, which affects or could affect the safety of
operations.”
2
All altitudes in this report are agl unless otherwise indicated.
3
Similarly, no crewmembers and passengers aboard the airplanes on taxiway C were injured, and none of those
airplanes were damaged.
4
Supporting documentation referenced in this report can be found in the public docket for this incident, accessible
from the National Transportation Safety Board’s (NTSB) Accident Dockets web page by searching DCA17IA148.
Other NTSB documents referenced in this report, including reports and summarized safety recommendation
correspondence, are accessible from the NTSB’s Aviation Information Resources web page (www.ntsb.gov/air).
5
Flight 759 was originally scheduled to push back from the gate at 1755 (2055 EDT), take off at 1809
(2109 EDT), and land at 2303 (0203 EDT).
6
The NTSB interviewed the incident captain on July 14 and the incident first officer on July 18, 2017. The NTSB
also interviewed both incident flight crewmembers on August 10, 2017.

NTSB Aircraft Incident Report
2
scan” of the NOTAMs in the flight release but could not recall whether he had seen the runway 28L
closure NOTAM and whether he and the captain had discussed the closure information at the gate.
The first officer also stated that he realized, after the incident flight landed, that runway 28L had
been closed. During an interview about 1 month after the incident, the captain stated that he and
the first officer had discussed the runway 28L closure while at YYZ but that they did not place
much emphasis on that information because, at that time, the flight was scheduled to land at SFO
before the runway would be closed. (The National Transportation Safety Board [NTSB] notes that
the flight was originally scheduled to land at SFO at 2303, 3 minutes after runway 28L was
scheduled to be closed.)
The airplane pushed back from the gate at YYZ at 1825 (2125 EDT), 30 minutes later than
originally scheduled. The captain was the pilot flying, and the first officer was the pilot monitoring.
Flight data recorder (FDR) data showed that the throttles were advanced to the takeoff power
setting about 1858 (2158 EDT) and that the autopilot was engaged shortly after takeoff and
remained engaged until just before the final approach to SFO.
7
The flight crewmembers reported
that the departure, climb, cruise, and descent phases of flight were uneventful except for an area
of thunderstorms about midway through the flight.
8
The crewmembers also reported that they
started to feel tired just after they navigated through the thunderstorms, which radar data indicated
was about 2145 (0045 EDT).
Before the airplane began its descent into the terminal area, the first officer obtained
automatic terminal information service (ATIS) information Quebec via the airplane’s aircraft
communication addressing and reporting system (ACARS) and printed the information.
9
(Air Canada records indicated that, about 2321, the airplane was sent the ACARS message with
the ATIS information.) Among other things, ATIS information Quebec indicated, “Quiet Bridge
visual approach in use,” “landing runway 28R,” and “NOTAMS…runways 28L, 10R closed.”
(SFO lighting logs indicated that the lights on runway 28L were turned off about 2312.) ATIS
information Quebec also indicated that the runway 28L approach lighting system and the
runway 28L/10R centerline lights were out of service. During postincident interviews, the flight
crewmembers recalled reviewing ATIS information Quebec but could not recall whether they saw
the ATIS-reported information about the runway 28L closure.
7
The airplane was equipped with a Honeywell solid-state FDR, model 980-4700-042, that was required by
14 CFR 129.20 to record 34 parameters and 25 hours of data. The FDR recording contained about 108 hours of data,
including 5 hours 15 minutes from the incident flight. The FDR recording for the incident flight began about 1835
(2135 EDT). The airplane was also equipped with a Honeywell solid-state cockpit voice recorder (CVR), model
980-6022-001, but the data from the incident flight were overwritten before Air Canada was notified about this
incident. (This CVR model was designed to record 2 hours of operational data, which was consistent with the
requirements of 14 CFR 129.5 and International Civil Aviation Organization Annex 6 for CVRs to retain the
information recorded during at least the last 2 hours of their operation.) Section 1.6.4 discusses notification events for
this incident.
8
During a postincident interview, the captain stated that it was “stressful” navigating through the area of
thunderstorms.
9
Air Canada allowed flight crews to obtain ATIS information using ACARS or VHF communications.

NTSB Aircraft Incident Report
3
ATIS information Quebec also included weather information.
10
Given this information and
the reported landing runway in use, the captain briefed Air Canada’s Flight Management System
(FMS) Bridge visual approach procedure to SFO runway 28R.
11
The FMS Bridge visual approach
to runway 28R, coded as the area navigation (RNAV) 28R approach, was a commercial airline
overlay chart (a Jeppesen chart customized for Air Canada) based on the Quiet Bridge visual
approach procedure to runway 28R.
12
Air Canada’s FMS Bridge visual approach procedure to runway 28R required pilots of
Airbus A319/A320/A321 airplanes to manually enter (tune) the instrument landing system (ILS)
frequency into the airplane’s flight management computer (FMC) to provide backup lateral
guidance (via the localizer) to the runway.
13
The FMS Bridge visual approach to runway 28R was
the only approach in Air Canada’s Airbus A320 database that required manual tuning for a
navigational aid.
14
As part of his pilot monitoring duties, the first officer would have used the
multifunction control and display unit (MCDU) to program required settings, but he did not enter
the ILS frequency into the radio/navigation page. The first officer reported, during a postincident
interview, that he “must have missed” the radio/navigation page and was unsure how that could
have happened. Also, the captain did not verify, during the approach briefing, that the ILS
frequency had been entered, and neither flight crewmember noticed that the ILS frequency was
not shown on the primary flight displays (PFD).
15
FDR data showed that the ILS frequency was
not tuned and that no frequency had been entered.
As part of the approach briefing, Air Canada’s procedures required the flight crew to
discuss any threats associated with the approach. The captain stated that they discussed as threats
the nighttime landing, the traffic, and the busy airspace. The captain also reported that he and the
first officer discussed that “it was getting late” and that they would need to “keep an eye on each
other.” The first officer stated that the threats were the mountainous terrain, the nighttime
10
ATIS information Quebec included the automated surface observing system weather information recorded at
2256. The ATIS information indicated the following: wind was from 310° at 12 knots, visibility was 10 statute miles,
sky was clear, temperature was 17°C (63°F), dew point was 9°C (48°F), and altimeter was 29.93 inches of mercury.
The automated surface observing system weather information at 2356 (the time of the incident) indicated the
following: wind was from 290° at 9 knots, visibility was 10 statute miles, sky was clear, temperature was 16°C (61°F),
dew point was 9°C (48°F), and altimeter was 29.92 inches of mercury.
11
The approach briefing is the first item on Air Canada’s pre-descent checklist.
12
Figure 9 in section 1.6.6 shows the approach chart.
13
According to the Federal Aviation Administration’s (FAA) Aeronautical Information Manual, section 1-1-9,
ILS ground equipment consists of two “highly directional transmitting systems,” one of which is the localizer, which
provides course guidance to the runway centerline. Air Canada’s chart for the FMS Bridge visual approach to
runway 28R showed the ILS frequency (111.7) in the plan view. The Jeppesen chart for the ILS or localizer approach
to runway 28R showed 111.7 as the localizer frequency.
14
Honeywell, the manufacturer of the Air Canada A320 FMS, stated, in e-mails dated July 19, 2018, that the
procedure for this approach was created by United Airlines and that Air Canada used United Airlines’ database for its
operations. The database did not include a frequency for the FMS to autotune for the approach procedure, and
Air Canada’s policy was to make changes to the database only if information (such as waypoints and altitude
restrictions) was not correct. Because the information that United Airlines developed for this approach did not include
a frequency for autotuning, manual tuning of the ILS was required.
15
For ILS information to appear on the PFDs, one of the incident flight crewmembers would have had to select
the “LS” buttons on the glareshield, but neither crewmember mentioned selecting this button during the approach.
Air Canada’s procedures for the FMS Bridge visual approach to runway 28R did not indicate that a flight crew was
required to take this action.

NTSB Aircraft Incident Report
4
conditions, and both flight crewmembers’ alertness. The captain and the first officer could not
recall whether they discussed the runway 28L closure during the approach briefing.
FDR data showed that, about 2324, the selected altitude for the autopilot changed from the
cruise altitude (flight level 360) to 8,000 ft mean sea level (msl), which was the crossing altitude
for the first waypoint on the approach. When the airplane began its descent about 2327, the
autopilot lateral navigation mode remained as “NAV [navigation],” and the vertical navigation
mode changed to “DES [descent].” According to Airbus, this configuration was consistent with
the autopilot operating in a managed descent profile.
16
According to air traffic control (ATC) voice recordings, at 2330:42, the flight crew checked
in with the Northern California terminal radar approach control (NCT) approach controller on the
DYAMD 3 (RNAV) standard terminal arrival route to SFO.
17
At that time, the airplane was
descending from an altitude of 27,000 ft msl.
After the flight crew’s initial contact with NCT, the controller issued instructions to join
the FMS Bridge visual approach to runway 28R after reaching the final waypoint on the standard
terminal arrival route. FDR data showed that, as the airplane descended through an altitude of
about 14,500 ft msl at 2336:30, the altitude selected parameter changed to 10,944 ft msl. At
2338:01, the autopilot lateral navigation mode changed from “NAV” to “HDG [heading]” with no
recorded corresponding change in the vertical navigation mode. According to Airbus, this
configuration and the change in selected altitude were consistent with the autopilot operating in an
open descent profile.
18
The flight crewmembers did not discuss the descent mode during the
approach briefing, but the first officer reported, during a postincident interview, that he perceived
that the descent mode had switched from a managed to an open descent.
19
The first officer also
stated that he was uncomfortable with the approach being flown in the open descent mode and that
he did not say anything to the captain because the procedure was allowed.
20
At 2346:08, the controller instructed ACA759 to turn right direct to the TRDOW waypoint
and join the FMS Bridge visual approach to runway 28R, and the flight crew acknowledged this
16
Air Canada’s A319/A320/A321 Aircraft Operating Manual, volume 1, section 4, “Standard Operating
Procedures,” indicated that, for the managed descent mode, an airplane is guided along the FMS lateral and vertical
flight plan and speed profile. For more information about this descent mode, see section 1.6.1.
17
The NTSB determined the time and content of air/ground transmissions referenced in this report using certified
FAA audio recordings of NCT and SFO air traffic control tower communications.
18
Air Canada’s A319/A320/A321 Aircraft Operating Manual indicated that, for the selected descent mode (also
referred to as the open descent mode), an airplane is guided by targets that the pilot flying selects and enters into the
flight control unit. For more information about this descent mode, see section 1.6.1. According to FDR data, between
the altitudes of 8,040 and 1,456 ft msl, the airplane could have been operating in either the open descent mode or the
managed descent mode without altitude constraints.
19
In an e-mail dated March 23, 2018, the captain stated the following about the descent mode: “The descent
initially was flown in selected [open mode] to catch up with the profile…[in] part due to the [air traffic] controller
taking us out of the normal approach and due to radar vectoring. Once I was comfortable that the airplane, and the
automation was caught up with the FMC, and the profile, the rest of the approach was flown in Managed mode as per
the profile published on the approach plate.” The NTSB notes that situations that might warrant the use of the open
descent mode include vectoring off the approach (which occurred during the incident flight), maintaining a specific
altitude that is above the glidepath until reaching a specific intersection, and descending to a certain altitude that is
below the projected calculated glidepath.
20
According to Air Canada, the procedure was allowed until reaching the final waypoint on the approach.

NTSB Aircraft Incident Report
5
instruction.
21
At 2346:19, the controller asked the crewmembers if they had the airport or bridges
in sight; the flight crew replied that the bridges were in sight. At 2346:30, the controller cleared
the airplane for the approach and, at 2350:48, instructed the flight crew to contact the SFO air
traffic control tower (ATCT).
At 2351:07, the flight crew contacted the SFO ATCT and advised that the airplane was on
the FMS Bridge visual approach to runway 28R. Four seconds later, the tower controller issued a
landing clearance for runway 28R.
22
The flight crew acknowledged the landing clearance at
2351:18. FDR data showed that the landing gear was selected to the down position at 2352:46.
Air Canada’s FMS Bridge visual approach procedure to runway 28R indicated that pilots
of Airbus A319/A320/A321 airplanes were to do the following: “at or before F101D [the final
waypoint on the approach], disengage autopilot and continue as per Visual Approaches [standard
operating procedures].” FDR data showed that the autopilot was disconnected at 2353:28 when
the airplane was at an altitude of 1,300 ft and that the flight directors were disengaged at 2354:02
when the airplane was at an altitude of 1,200 ft. The airplane passed F101D at 2354:28, when the
airplane was at an altitude of about 1,100 ft, and the captain made the required 14° right turn to
align the airplane with runway 28R but instead aligned the airplane with taxiway C.
During a postincident interview, the first officer reported that, during the approach, he was
looking inside the cockpit to accomplish his tasks as the pilot monitoring. For example, after the
autopilot was disconnected, the first officer set the missed approach altitude and heading in case a
missed approach was necessary; the first officer stated that he had to look at the approach chart to
obtain that information. Also, the first officer reported that the captain had asked him to set the
heading bug (indicator) to the runway heading. The first officer stated that he had difficulty finding
the heading information on the approach chart, so he had to reference the airport chart.
23
The
captain reported that he saw lights across what he thought was the runway 28R surface. The captain
asked the first officer to find out whether the runway was clear, at which time the first officer
looked outside the cockpit. The first officer stated that the captain’s request occurred between the
time that the airplane passed F101D (at an altitude of about 1,100 ft) and the time that the airplane
descended to an altitude of 600 ft.
The ATC voice recording indicated that, at 2355:45, the flight crew made the following
transmission to the controller: “Just want to confirm, this is Air Canada seven five nine, we see
some lights on the runway there, across the runway. Can you confirm we’re cleared to land?”
24
At
that time, the airplane was passing through an altitude of 300 ft. During a postincident interview,
the controller stated that, just before the query about the status of runway 28R, he had visually
scanned the runways from the departure to approach ends. The controller also stated that, in
21
Once the airplane joined the approach, the autopilot lateral navigation mode changed to “NAV.”
22
The tower controller was working all positions in the ATCT at that time. Section 1.4.1 discusses ATCT staffing
on the night of the incident.
23
FDR data indicated that the missed approach altitude and the runway heading were set at 2355:00.
24
The captain stated, during a postincident interview, that it took “a while” for the first officer to contact the
controller because of “chatter” on the tower frequency. The ATC voice recording showed that, during the 61 seconds
before the flight crew’s query to the controller, there were ongoing communications between the tower and airplanes
on the ground.
NTSB Aircraft Incident Report
6
response to the query, he checked the radar display and the airport surface surveillance capability
(ASSC) display and then rescanned runway 28R. Regarding the ASSC display, the controller
reported that he saw the ACA759 data symbol just to the right of the runway centerline, which he
stated was normal for the FMS Bridge visual approach to runway 28R.
At 2355:52, 1 second after the flight crew completed its transmission, the controller replied,
“Air Canada seven five nine confirmed cleared to land runway two eight right. There’s no one on
runway two eight right but you.”
25
About that time, the airplane was passing through an altitude
of 200 ft and was 2,300 ft (0.38 nautical mile [nm]) from the seawall that protected the airfield
from San Francisco Bay.
26
At 2355:58, the flight crew acknowledged the transmission; about that
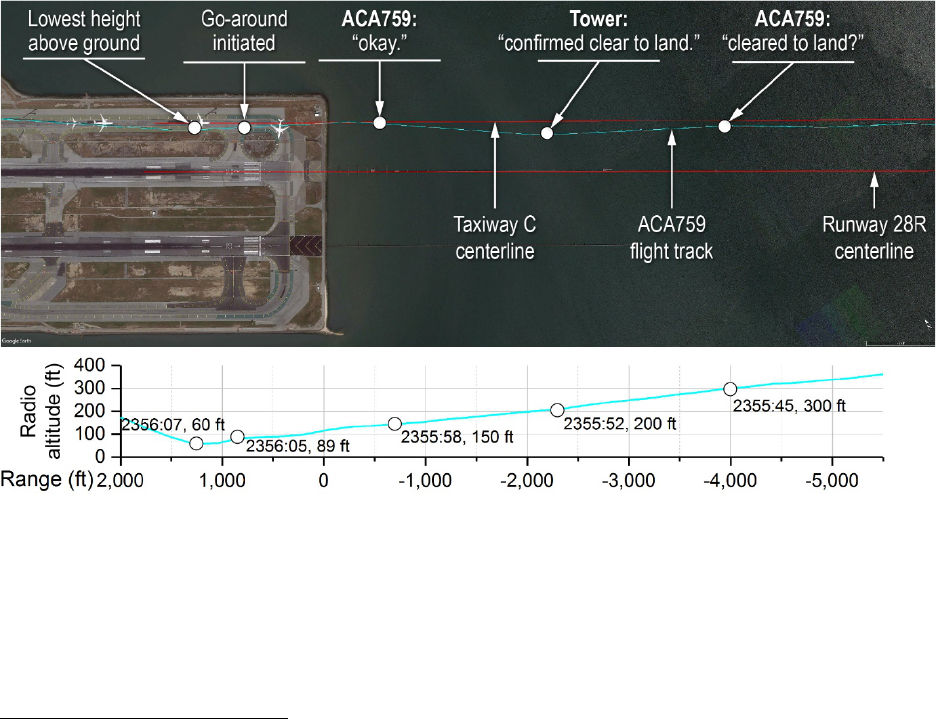
time, the airplane was 500 ft (0.08 nm) from the seawall. Figure 1 shows ACA759’s track before
reaching the seawall along with the extended centerlines for runway 28R and taxiway C.
Figure 1. ACA759 track over SFO.
Note: (a) This figure shows a plot of data and does not depict information that was available to the pilots and controller.
(b) The range shown at the bottom of the figure is the distance from/beyond the airport seawall.
25
At this time, the ACA759 data symbol (which showed only the airplane’s call sign) disappeared from the ASSC
display because the airplane was no longer in the system’s depiction area (coverage cone). The ASSC display showed
the ACA759 data symbol again 12 seconds later, at 2356:04. For more information about the ASSC system, see
section 1.4.2.
26
The seawall was about 650 ft from the runway 28R displaced threshold and about 400 ft from the paved surface
of taxiway C. Because taxiway C did not have a defined threshold (the taxiway curved when intersecting runway 28R),
the seawall located before the approach ends of runways 28R and 28L was used to reference distances during the
incident airplane’s approach to taxiway C.

NTSB Aircraft Incident Report
7
The ATC voice recording also indicated that, at 2355:59, another pilot stated on the tower
frequency, “where is that guy going?”
27
The voice on the transmission was later identified as that
of the captain from the first airplane on taxiway C, United Airlines flight 1 (UAL1). About that
time, ACA759 was still 500 ft (0.08 nm) from the airport seawall and at an altitude of 150 ft while
lined up with taxiway C. At 2356:03 (after ACA759 crossed the seawall), ACA759 overflew
UAL1 at an altitude of 100 ft; about the same time, the UAL1 captain stated, over the tower
frequency, “he’s on the taxiway.” About the same time as the UAL1 captain’s second transmission,
the flight crew from the second airplane on taxiway C, Philippine Airlines flight 115 (PAL115),
turned on that airplane’s landing gear and nose lights, illuminating a portion of the taxiway and
the UAL1 airplane.
FDR data showed that, at 2356:05, the throttles on ACA759 were advanced, and the
airplane’s engine power and pitch increased. At that time, the airplane was at an altitude of about
89 ft.
28
During a postincident interview, the captain stated that, as the airplane was getting ready
to land, “things were not adding up” and it “did not look good,” so he initiated a go-around.
29
The
captain reported that he thought that he saw runway lights for runway 28L and believed that
runway 28R was runway 28L and that taxiway C was runway 28R.
30
During a postincident
interview, the first officer reported that he thought that he saw runway edge lights but that, after
the tower controller confirmed that the runway was clear, he then thought that “something was not
right”; as a result, the first officer called for a go-around because he could not resolve what he was
seeing. The captain further reported that the first officer’s callout occurred simultaneously with
the captain’s initiation of the go-around maneuver.
The airplane continued descending, reaching a minimum altitude of about 60 ft at 2356:07
as the airplane overflew PAL115. One second later, once the engines and elevators had fully
transitioned to their go-around position, the airplane began to climb. During the 3 seconds between
the time that the flight crew initiated the go-around and the airplane began climbing, ACA759 had
flown about 700 ft (0.12 nm) from the location over the taxiway where the go-around was initiated.
27
The controller stated, during a postincident interview, that the transmission seemed “out of context.” The ATC
voice recording indicated that, 2 seconds after this transmission, the controller stated to himself, “who is…talk?”
28
The NTSB performed an airplane performance study for this incident (see section 1.5.1), and some
FDR-recorded altitudes were adjusted according to the results of the study. For example, the airplane’s altitude when
the throttles were advanced was adjusted from the FDR-recorded radio altitude (which indicates the airplane’s height
above the ground) of about 84 ft. Also, the airplane’s FDR-recorded minimum altitude of 59 ft (at 2356:07) was
adjusted.
29
Air Canada’s Flight Operations Manual provided the criteria regarding when a go-around should be initiated.
These criteria included “landing will not be accomplished within the touchdown zone” and “landing will not be
accomplished on the runway centerline.” The captain stated, during a postincident interview, that he thought that the
go-around maneuver began when the airplane was at an altitude of about 400 ft and was 0.5 nm from the runway. The
NTSB determined the initiation of the go-around (at an altitude of 89 ft and 0.26 nm beyond the seawall) by the throttle
lever angles, which increased from 22.5° to 42°; the engine N1 (fan speed), which increased from 57 to 94%; and the
corresponding sidestick input as the throttles were advanced.
30
Between the time of the runway 28L closure and ACA759’s approach, nine airplanes flew the FMS Bridge
visual approach and made uneventful landings on runway 28R. (Four airplanes were on taxiway C during that time,
as described in this section.) The pilots of the flight that immediately preceded ACA759 reported confusion regarding
the identification of the runway 28R surface, as discussed in section 1.1.1.
NTSB Aircraft Incident Report
8
At 2356:09, the controller instructed the ACA759 flight crew to go around.
31
The ACA759
flight crew acknowledged this instruction 2 seconds later as the airplane overflew the third airplane
on the taxiway, United Airlines flight 863 (UAL863), at an altitude of 200 ft. Immediately
afterward, ACA759 overflew the fourth airplane on the taxiway, United Airlines flight 1118
(UAL1118) at an altitude of 250 ft. Both incident pilots reported (during postincident interviews)
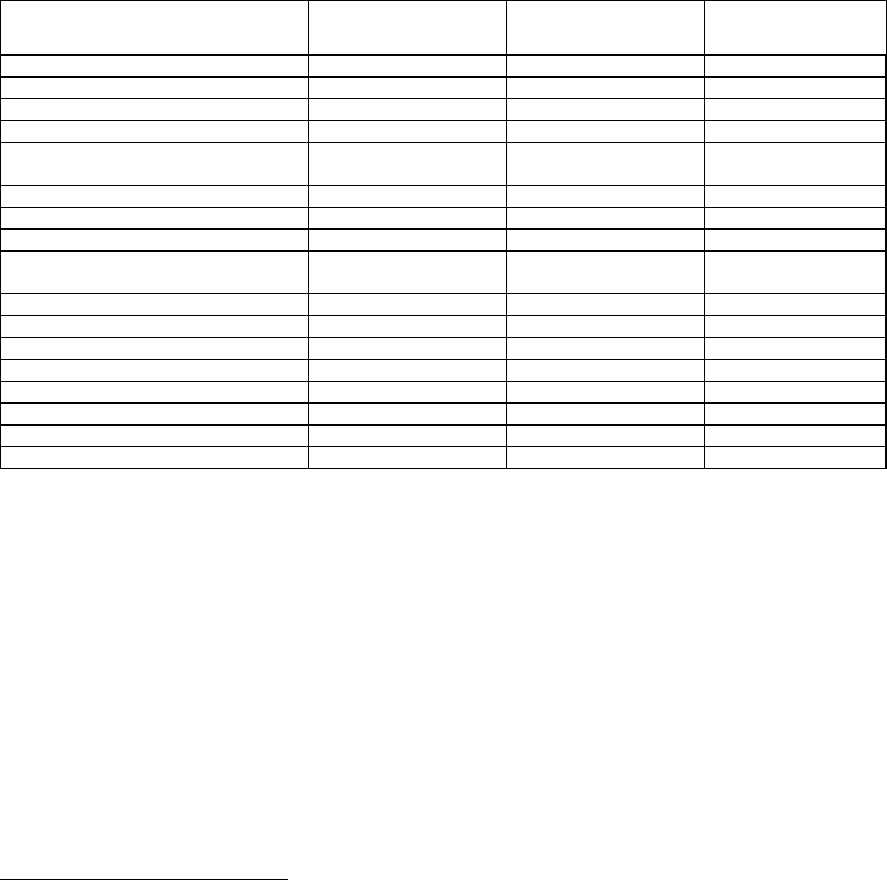
that they did not see any airplanes on the taxiway. Table 1 shows the events between ACA759’s
landing clearance and overflight of taxiway C according to the airplane performance study
conducted for this incident.
Table 1. Timeline of events.
Event Time
Distance from
airport seawall
Airplane altitude
(agl)
Tower: Cleared to land 28R.
2351:11
-11.5 nm
3,500 ft
Landing gear down
2352:46
-7.7 nm
2,000 ft
Autopilot off
2353:28
-6.0 nm
1,300 ft
Flight directors off
2354:02
-4.8 nm
1,200 ft
Passed F101D and lined up with
taxiway C
2354:28
-3.6 nm
1,100 ft
ACA759: Confirm runway clear.
2355:45
-4,000 ft, -0.66 nm
300 ft
Tower: Confirmed clear to land.
2355:52
-2,300 ft, -0.38 nm
200 ft
ACA759: Okay.
2355:58
-500 ft, -0.08 nm
150 ft
UAL1 pilot: Where is that guy
going?
2355:59
-500 ft, -0.08 nm
150 ft
UAL1 pilot: He’s on the taxiway.
2356:03
+450 ft, +0.07 nm
100 ft
Passed over UAL1
2356:03
+450 ft, +0.07 nm
100 ft
Throttles advanced for go-around
2356:05
+850 ft, +0.11 nm
89 ft
Passed over PAL115
2356:07
+1,250 ft, +0.21 nm
60 ft
Began climb
2356:08
+1,550 ft, +0.26 nm
89 ft
Tower: Go around.
2356:09
+1,700 ft, +0.28 nm
130 ft
Passed over UAL863
2356:11
+2,200 ft, +0.36 nm
200 ft
Passed over UAL1118
2356:12
+2,600 ft, +0.43 nm
250 ft
Note: The airplane’s distance from the seawall is expressed in feet and nautical miles for distances less than 1 nm.
At 2356:12, the controller advised the ACA759 flight crew, “it looks like you were lined
up for [taxiway] Charlie,” and instructed ACA759 to fly a heading of 280° and climb to 3,000 ft
msl. The flight crew acknowledged the heading and altitude instructions at 2356:18. At 2356:23,
ACA759’s landing gear was raised; 5 seconds later, the autopilot was engaged. At 2356:44 and
2356:55, the controller instructed the flight crew to contact NCT, and the crew acknowledged the
instruction at 2357:00. During the downwind leg for ACA759’s second approach, the first officer
asked the captain if they should set the ILS frequency, and the captain agreed. The second approach
to SFO was uneventful, and ACA759 made a successful landing on runway 28R about 0011 on
July 8. The captain and first officer completed their duty periods at 0032.
31
(a) The controller stated that, when ACA759 was about 1/10 mile on short final, he noticed that the airplane
looked “extremely strange” regarding its proximity to taxiway C and the airplanes on the taxiway and then made the
decision to have ACA759 go around. (b) The flight crewmembers indicated, during postincident interviews, that they
did not hear specific transmissions on the tower frequency between the controller’s verification that the runway was
clear and his go-around instruction.

NTSB Aircraft Incident Report
9
1.1.1 Preceding Arrival on Runway 28R
The airplane that preceded the incident airplane into SFO, a Boeing 737 operated as Delta
Air Lines flight 521 (DAL521), landed on runway 28R about 4 minutes before the incident
occurred. During postincident interviews, both DAL521 flight crewmembers reported that, after
visually acquiring the runway environment, they questioned whether their airplane was lined up
for runway 28R.
32
The DAL521 captain stated that he could see lights (but no airplanes) on
taxiway C and that those lights gave the impression that the surface could have been a runway.
33
The DAL521 first officer reported seeing a set of lights to the right of runway 28R but that he
“could not register” what those lights were. The DAL521 first officer also reported that there were
“really bright” white lights on the left side of runway 28R (similar to the type used during
construction), but both he and the captain knew that runway 28L was closed.
The DAL521 flight crewmembers were able to determine that their airplane was lined up
for runway 28R after cross-checking the lateral navigation (LNAV) guidance. The DAL521
captain stated that, without lateral guidance, he could understand how the runway 28R and
taxiway C surfaces could have been confused because the lights observed on the taxiway were in
a straight line and could have been perceived as a centerline. The DAL521 crewmembers
confirmed that their airplane was lined up correctly when they visually acquired the painted “28R”
marking on the paved surface of the runway; they estimated that their airplane was at an altitude
of 300 ft at that time.
34
The DAL521 captain and first officer provided written statements to Delta Air Lines (dated
July 13 and 12, 2017, respectively) that were subsequently provided to the NTSB. The DAL521
captain stated, “had the runway sequenced flashing lights been on it would have defined the
landing runway or had we flown the ILS [approach] we would have had precision course guidance
which would have eliminated the illusion that we were not lined up on runway 28R.” The DAL521
first officer stated, “the PF [pilot flying] stayed on the LNAV guidance all the way to the runway
which mitigated the confusion we experienced from the lighting and non-normal airport
configuration at SFO that night.”
35
Both flight crewmembers indicated that, after landing, they
heard a radio communication about an airplane lined up with the taxiway followed by the tower
controller’s instruction for the airplane to go around, and the first officer indicated that he saw an
aircraft lined up on the taxiway initiating a go-around. The DAL521 first officer also indicated that
he called the ATCT about 40 to 50 minutes after the incident and suggested that, to assist pilots
32
Similar to the ACA759 flight crew, the DAL521 flight crew flew the FMS Bridge visual approach to
runway 28R.
33
The ASSC system showed that, as DAL521 approached the runway, UAL1, PAL115, UAL863, and UAL1118
were on the taxiway (in about the same positions as when ACA759 approached the runway).
34
The airplane performance study showed that, when the incident airplane reached an altitude of 300 ft, the
airplane was 4,000 ft (0.66 nm) from the seawall, so the DAL521 airplane was most likely about the same distance
from the seawall when the DAL521 flight crew visually acquired the painted “28R” on the runway.
35
The DAL521 first officer also stated the following: “The construction lights were so bright we could not
determine the location of the inboard runway, 28L. So I initially thought the construction was on a taxiway and we
might be lined up on Rwy 28L and the taxiway on the right could be Rwy 28R.”

NTSB Aircraft Incident Report
10
with runway identification, flight crews should “fly ILS approaches to RWY 28R” or the tower
should “turn on the lights for RWY 28L.”
36
1.1.2 Airplanes on Taxiway C
The flight crews of the four airplanes that were on taxiway C at the time of the incident
provided written statements to the NTSB. The captain of the first airplane, a Boeing 787 operated
as UAL1, stated that he had a clear view of arriving traffic. The UAL1 captain also stated that he
first saw ACA759 when it was about 1 to 2 miles away because ACA759’s landing lights were
pointed directly at the UAL1 airplane. He thought that ACA759 would correct its course and align
with the runway. When that did not occur, he transmitted “where is that guy going” and “he’s on
the taxiway” on the tower frequency, and the controller directed the incident airplane to go around.
The flight crewmembers of the second airplane, an Airbus A340 operated as PAL115,
stated that, when ACA759 was on short final, it became evident that the airplane was lined up with
taxiway C. The PAL115 crewmembers also reported that they switched on their airplane’s landing
gear lights and nose lights so that the ACA759 flight crewmembers could recognize that they had
aligned the airplane with a taxiway. The PAL115 crewmembers further stated that the controller’s
go-around instruction was issued after ACA759 had overflown their airplane.
The captain of the third airplane, a Boeing 787 operated as UAL863, stated that he turned
on all airplane lights before the ACA759 flight crew performed a go-around. The UAL863
first officer stated that “a lot of lights” were on runway 28L and that he noticed an “X” on
runway 28L.
37
The UAL863 first officer also stated that it “quickly became obvious” that ACA759
was lining up with the taxiway. One of the UAL863 relief first officers (who was in the cockpit at
the time) stated that “the tower controller should not have been the only controller working the
entire airport” because it took him a few seconds to respond to the UAL1 pilot’s transmissions.
The captain of the fourth airplane, a Boeing 737 operated as UAL1118, stated that he lost
sight of ACA759 when it was at an altitude of about 500 to 600 ft because of his airplane’s position
behind a Boeing 787. The captain also stated that, although the ACA759 flight crew “made a
serious mistake that went unchecked for way too long,” it was also important to note that the tower
controller “was performing way too many functions…Ground, Tower, and at times ops vehicles.”
1.2 Personnel Information
1.2.1 The Captain
The captain, age 56, held a Canadian airline transport pilot (aeroplane) license with a
multiengine land rating. The captain’s most recent pilot’s license, dated October 2, 2015, included
a type rating for the EA32, which is the Canadian flight crew type rating designation for
36
During a postincident interview, the controller stated that, after ACA759 landed, a pilot from a Delta Air Lines
flight called the tower to report a problem differentiating runway 28R from taxiway C.
37
The incident flight crewmembers stated that they did not see a lighted “X” on runway 28L to indicate that it
was closed. Similarly, neither DAL521 pilot recalled seeing a lighted “X” to indicate that runway 28L was closed.

NTSB Aircraft Incident Report
11
Airbus A320-series airplanes. The captain also held a category 1 medical certificate dated
December 20, 2016, with a limitation that required him to wear glasses.
38
The captain reported
that he was wearing his glasses at the time of the incident.
The captain was employed by Canadian Airlines between 1988 and 2000 and Air Canada
since 2000 (after the two airlines merged). He had been a captain on the A320 since 2007.
According to Air Canada records and information provided by the captain, he had accumulated
about 20,000 hours of total flight experience, including about 7,063 hours in the A320, about
4,797 hours of which were as an A320 pilot-in-command. He had flown about 166, 56, 11, and
6 hours in the 90, 30, and 7 days and 24 hours, respectively, before the incident. The captain’s last
line check occurred on March 8, 2017, and his last recurrent ground training occurred on
January 20, 2017. The captain had no previous accident or incident history, and company training
records showed that he had not failed any pilot checkrides.
The captain reported that he had been to SFO “lots of times,” including once or twice
during the 4 months before the incident. The captain recalled that, on previous flights into SFO,
runways 28L and 28R were both illuminated, and he stated that he had never seen runway 28L
“dark.” The incident flight was the first time that the captain and the first officer had flown
together.
72-Hour History
The captain stated that he went to sleep between 0030 and 0100 EDT on July 5, 2017, and
awoke between 0700 and 0800 EDT. He was off from work that day. On July 6, the captain went
to sleep about 0000 EDT and awoke about 0800 EDT. The captain was a reserve pilot for
Air Canada, and his reserve duty period on July 6 began at 0500 EDT. He reported for duty
between 1600 and 1700 EDT and flew to LaGuardia Airport, New York, New York, and then back
to YYZ. He went off duty at 2313 EDT (15 minutes after the flight arrived at the gate) and then
cleared customs, took a train to the airport parking lot, walked to his car, and drove home. He
stated that the flight from New York, because of its arrival time, affected his sleep cycle “a little
bit.” The captain went to sleep between 0200 and 0300 EDT on July 7 and awoke about 0745 EDT.
The captain considered himself to be “fairly rested” during the 3 nights before the incident flight.
The captain’s reserve duty period began at 1113 EDT on July 7. About 1149 EDT, crew
scheduling called the captain to notify him of a round-trip flight assignment from YYZ to SFO.
39
The captain did not take any naps that day and reported for duty by 1940 EDT. The captain
considered himself to be rested before the flight but reported that he started feeling fatigued
midway through the flight, just after the airplane maneuvered through an area of thunderstorms.
At the time of the incident, the captain had been awake for more than 19 hours. Table 2 shows the
captain’s sleep schedule during the 72 hours before the incident.
38
The Transportation Safety Board of Canada reviewed both flight crewmembers’ medical certificates as part of
this investigation and found that the captain and the first officer reported no medications, medical conditions, or sleep
disorders as part of their category 1 medical examinations. In addition, neither flight crewmember reported any
medications, medical conditions, or sleep disorders during postincident interviews.
39
The return flight, from SFO to YYZ, departed on July 8 at 1649 (1949 EDT) and arrived at 2135 (0035 EDT
on July 9).

NTSB Aircraft Incident Report
12
Table 2. Captain’s self-reported sleep schedule.
Date Bedtime (EDT) Awakening time (EDT) Sleep opportunity
July 4 to 5
Between 0030 and 0100
Between 0700 and 0800
6 to 7.5 hours
July 5 to 6
0000
0800
8 hours
July 6 to 7
Between 0200 and 0300
0745
4.75 to 5.75 hours
The captain stated that he normally obtained between 6 and 7 hours of sleep each night and
felt rested after that amount of sleep. He consistently went to bed after 0000 EDT and considered
himself to be neither a morning nor an evening person. The captain thought that it was “hard to
get into a rhythm” when traveling because of difficulty winding down and falling asleep
immediately after flights. The captain reported that he did not take any prescription or
nonprescription medicine, use tobacco products or illicit drugs, and consume alcohol in the
72 hours before the incident. The captain also reported no issues with his health and had no changes
to his health, financial situation, or personal life within the 12 months before the incident that
would have affected his performance on the day of the incident.
1.2.2 The First Officer
The first officer, age 42, held a Canadian airline transport pilot (aeroplane) license with a
multiengine land rating. The first officer’s most recent pilot’s license, dated November 30, 2015,
included a type rating for the EA32 (the Canadian flight crew type rating designation for Airbus
A320-series airplanes). The first officer also held a category 1 medical certificate dated May 12,
2017, with no limitations.
The first officer had been employed by Air Canada since December 2007. According to
Air Canada records and information provided by the first officer, he had accumulated about
10,000 hours of total flight experience, including about 2,343 hours in the A320 as
second-in-command. He had flown about 148, 70, 18, and 6 hours in the 90, 30, and 7 days and
24 hours, respectively, before the incident. The first officer’s last line check occurred on April 25,
2017, and his last recurrent ground training occurred on December 29, 2016. The first officer had
no previous accident or incident history.
The first officer reported that he had twice attempted to upgrade to A320 captain.
Air Canada records showed that the first officer passed his command line operational evaluation
training on February 6 and 7, 2017, and that he did not pass his qualifying oriented evaluation
training on March 1 and 16, 2017. According to the simulator instructors and check airmen who
conducted the first officer’s upgrade attempts, the first officer had occasional difficulty
maintaining situational awareness and did not perform in accordance with required
Transport Canada standards.
40
Air Canada’s director of safety and training stated that the first
officer subsequently completed requalification training for the first officer position. The instructor
who administered this training stated that the first officer performed “above average.”
40
A check airman who flew with the incident first officer (when he was attempting to upgrade to captain) stated
that, during a flight, the incident first officer did not anticipate a potential flap overspeed event and respond to an
increase in thrust that would have caused a flap overspeed. The instructor stated that he had to intervene before a flap
overspeed occurred.
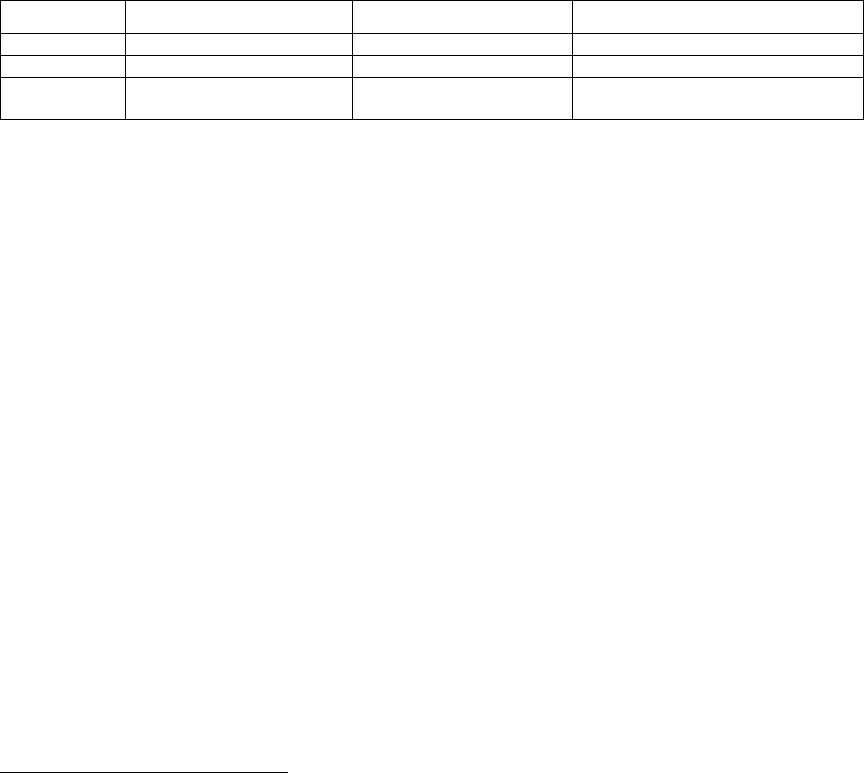
NTSB Aircraft Incident Report
13
72-Hour History
The first officer was off duty on July 4, 2017, and reported that he had a “proper” night’s
sleep then. On July 5, the first officer awoke about 0800 EDT and took a nap in the afternoon for
90 minutes. He was a flight crewmember (the pilot flying) that night for a flight to SFO, which
landed at 2305 (0205 EDT on July 6).
41
The first officer went to sleep about 0400 EDT and awoke
about 1000 EDT. He took a 1-hour nap in the afternoon and flew back to YYZ that night. The
flight arrived on July 7 about 0030 EDT, and the first officer went to sleep about 0300 EDT. He
awoke about 0900 EDT, took a 90-minute nap about 1300 EDT, and reported for duty at 1910 EDT
(30 minutes before the scheduled report time). The first officer stated that both he and the captain
began to feel “very tired” between 2330 and 0000 (0230 and 0300 EDT on July 8).
42
At the time
of the incident, the first officer had been awake for more than 12 hours. Table 3 shows the first
officer’s sleep schedule during the 72 hours before the incident.
Table 3. First officer’s self-reported sleep schedule.
Date Bedtime (EDT) Awakening time (EDT) Sleep opportunity
July 4 to 5
Unknown
Unknown
Unknown
July 5 to 6
0400
1000
6 hours plus 1-hour nap (7 hours)
July 6 to 7
0300
0900
6 hours plus 1.5-hour nap
(7.5 hours)
The first officer thought that he needed 8 hours of sleep each night to feel rested and
considered himself to be a “pretty heavy sleeper.” He also considered himself to be a “normal day
person” and stated that he typically felt tired about 2300 EDT. He normally took a nap in the
afternoon for about 90 minutes on the days that he was scheduled for a nighttime flight. The first
officer reported that he slept well during naps and felt rested afterward.
The first officer reported that he did not take any prescription or nonprescription medicine
in the 72 hours before the incident that would have affected his performance. The first officer also
reported that he did not use tobacco products or illicit drugs and that his last alcohol consumption
before the incident was dinnertime on either July 3 or 4. He further reported no issues with his
health and had no changes to his health, financial situation, or personal life within the 12 months
before the incident that would have affected his performance on the day of the incident.
1.3 Airplane Information
The incident airplane, shown in figure 2, was owned by GE Capital Aviation Services,
which leased the airplane to Air Canada. The airplane’s transport-category airworthiness
certificate was dated January 17, 1992. The airplane was powered by two CFM56-5A1 engines
and had 2 flight crew seats, 1 jumpseat, 5 cabin crew seats, and 154 passenger seats. The airplane’s
last inspection before the incident occurred on June 25, 2017, at which time the airplane had
accumulated a total of 82,427 hours of flight time.
41
SFO lighting logs showed that runway 28L closed at 2323 on July 5.
42
As indicated in section 1.1, the flight crewmembers also reported feeling tired just after they maneuvered the
airplane through the thunderstorms.

NTSB Aircraft Incident Report
14
Source: Air Canada.
Figure 2. Incident airplane.
1.4 Airport Information
SFO was located 8 miles southeast of San Francisco at an elevation of 13 ft msl. The airport
was owned and operated by the city and county of San Francisco and was certificated under
14 CFR Part 139. SFO had four runways (two sets of parallel runways) designated as 10L/28R,
10R/28L, 1R/19L, and 1L/19R, as shown in figure 3. Runway 10L/28R was 11,870 ft long and
200 ft wide. Runway 10R/28L was 11,381 ft long and 200 ft wide. Runway 28R was equipped
with a localizer that was aligned with the 284° runway heading. Taxiway C, which was to the right
of runway 28R (as viewed from the approach end of the runway), was 12,330 ft long and 75 ft
wide.
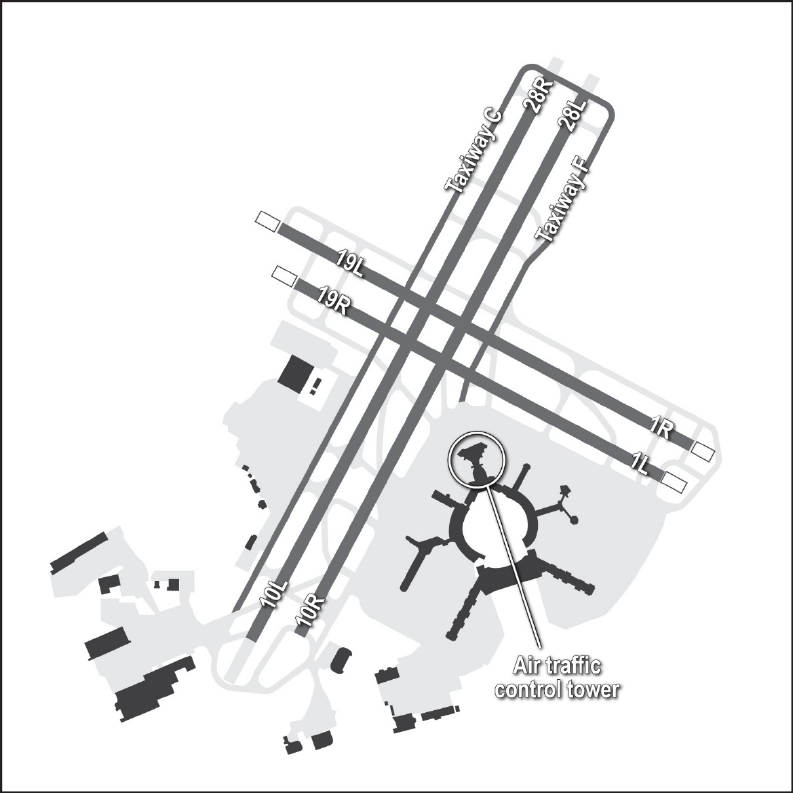
NTSB Aircraft Incident Report
15
Figure 3. SFO layout map.
The SFO inspection log showed the runway, taxiway, signage, and lighting inspections
surrounding the time of the incident. On July 7, 2017, runway 28R was inspected at 1550,
runway 28L was inspected at 1609, and all taxiways were inspected at 2108. On July 8, the airport
signage was inspected at 0211, and the airport lighting was inspected at 0339. No discrepancies
were noted for any of these inspections.
Title 14 CFR 139.311, “Marking, Signs, and Lighting,” stated that “each certificate holder
must provide and maintain lighting systems for air carrier operations when the airport is open at
night.” The regulation required runway and approach lighting that met specifications for takeoff
and landing minimums. The regulation also required that taxiways have one of four lighting
systems, one of which was centerline lights.
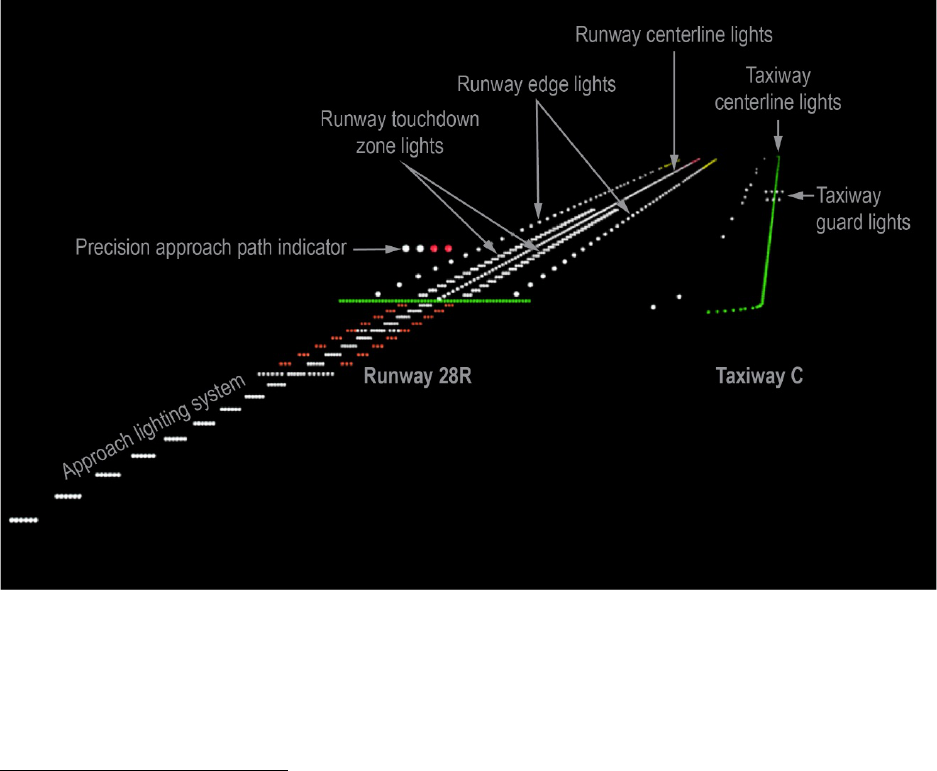
NTSB Aircraft Incident Report
16
The airport light status (on/off) and intensity were controlled from the ATCT. Runway 28R
was equipped with white runway edge lights, white centerline lights, white touchdown zone lights,
and an approach lighting system with white centerline sequenced flashing lights (ALSF-2).
43
Runway 28R was also equipped with a four-light precision approach path indicator with a
3° glidepath that was located on the left side of the runway. Taxiway C was equipped with green
centerline lights that were spaced at 50-ft intervals (± 5 ft), blue taxiway edge lights located at the
intersections with runway 28R to highlight the edge of the intersections, and flashing yellow
in-pavement guard lights located where taxiway C intersected runway 1R/19L (which ran
perpendicularly to runways 28L and 28R and taxiway C).
44
Figure 4 shows an illustration of the
lighting on runway 28R and taxiway C. On the night of the incident flight, the runway and taxiway
centerline lights were set at step 1 (out of 5).
Figure 4. Illustration of SFO’s lighting configuration.
Note: The green runway threshold lights (for runway 28R) are also shown.
Figure 4 also shows the ALSF-2 approach lighting system installed on runway 28R. The
approach lighting system had a total of 24 white centerline bar lights that were spaced at 100-ft
43
(a) An approach lighting system is a ground reference aid for pilots when making an approach to a runway.
(b) The runway centerline lights were white until the last 3,000 ft of the runway. From 3,000 to 1,000 ft, the color of
the lights alternated between red and white. For the last 1,000 ft, all of the lights were red. (c) The runway edge lights
transitioned from white to amber for the last 2,000 ft of the runway.
44
(a) During postincident interviews, the flight crewmembers recalled seeing specific color cues, including the
green taxiway centerline lights, while on approach to SFO. (b) The taxiways at YYZ had green centerline lights that
were spaced at 15-m (about 50-ft) intervals, retroreflective markers on the straight edges of the taxiways, and blue
edge lights around turns and at intersections.

NTSB Aircraft Incident Report
17
intervals and faced the direction of approaching aircraft, and 15 of the white centerline bar lights
extended into San Francisco Bay. Sequenced flashing lights (strobes) were positioned on the
15 centerline bar lights that were farthest from the runway to create, when the sequenced flashing
lights were turned on, the appearance of a rapidly moving light toward the runway.
45
During
postincident interviews, the tower controller who handled the incident flight stated that, on the
night of the incident, the approach lighting system was on, and the DAL521 captain stated that the
sequenced flashing lights were not on.
The purpose of the construction project on runway 10R/28L at the time of the incident was
to resurface the runway and replace existing light fixtures with improved lighting.
46
The project
started in February 2017 and was expected to last about 10 months.
47
The work required the
closure of the runway each night and during some weekends. At the time of the incident,
28 portable light plants were located around the construction zone.
48
A runway closure marker (a
white flashing lighted “X”) was placed at the approach and departure ends of runway 28L when
the runway was closed. The lighted “X” was 20.5 ft by 20.5 ft and flashed on for 2.5 seconds and
then off for 2.5 seconds, which was consistent with Federal Aviation Administration (FAA)
Advisory Circular (AC) 150/5345-55A, “Specification for L-893, Lighted Visual Aid to Indicate
Temporary Runway Closure.”
49
The flashing light associated with the “X” on runway 28L could
be seen on an SFO security video that captured the incident. (See section 1.5.1 for information
about the video).
One of the controllers at the SFO ATCT stated, during a postincident interview, that he had
noticed an increase in pilot requests to adjust the lights for runway 28R due to the construction on
runway 28L. According to the SFO acting air traffic manager, after the incident, controllers at the
SFO ATCT were directed to (1) increase the intensity of the approach lights by one step if the
adjacent arrival runway is closed and (2) when construction is ongoing, ask the pilots of the first
arriving airplane after dark if the construction lighting is distracting.
45
Controllers normally select a lighting setting based on the weather conditions. On the night of the incident, the
weather was VMC, so the sequenced flashing (strobe) lights would not have been on (unless a pilot requested them).
46
The replacement lighting included new runway-to-taxiway lead-on/lead-off lights, takeoff hold lights, and
runway entrance lights.
47
The runway 10R/28L project was completed on December 18, 2017.
48
Each light plant extended up to 30 ft and included four elliptical light fixtures that used 1,000-watt halide light
bulbs.
49
The L-893 runway closure marker currently in use in the national airspace system was intended for short-term
closures. This marker resulted from a research project conducted at the FAA Technical Center, the results of which
were published in a January 1987 technical report. According to the report, the development of a lighted visual aid to
denote closed runway surfaces included the following performance criteria: (1) the visual aid should be conspicuous
when viewed from the air with and without other runway visual aids illuminated, (2) the visual aid should be visible
from any point 0.5 mile from the runway threshold, (3) the visual aid should be suitable for night operations down to
a visibility of 3 miles, and (4) the message presented by the visual aid should be intuitively understood (Marinelli
1987). Various lighted visual aids were considered during this research project, and a lighted “X” was selected for
evaluation. A similar lighted visual aid had been in operational use at SFO at that time, which “reinforced results”
from the FAA Technical Center’s evaluation. The NTSB is not aware of any further FAA research for the L-893
runway closure markers (after their implementation) except for assessing the use of light-emitting diode bulbs.

NTSB Aircraft Incident Report
18
1.4.1 Air Traffic Control Tower Staffing
The SFO ATCT operated 24 hours a day. At the time of the incident, the ATCT was staffed
with two controllers who were assigned to the midnight shift (2230 to 0630). The controller
handling the incident flight had been an FAA controller since December 2008 and had been
working at the SFO ATCT since 2013. He was qualified and current on all positions at SFO and
was designated as a controller-in-charge.
50
The controller had also worked a daytime shift on
July 7 from 0530 to 1330. The controller reported that he took a 45-minute nap in between the
morning and midnight shifts and that he felt rested for his shifts.
51
The controller also stated that
he had “no problems” adjusting to the midnight shift.
The controller reported to the tower at 2230 on July 7 and initially worked the ground
control position. (The other controller assigned to the midnight shift was initially working the local
control position.) The front-line manager had briefed both controllers about the closure of
runway 28L at 2300. About 2349, all ATCT positions and frequencies had been combined, and
one controller worked the positions in the tower cab while the other controller took a recuperative
break in the building.
52
The controller who worked all positions configured his workstation to hear
the SFO local control (tower) frequency and NCT interphone communications through his headset
and the SFO ground control frequency over the workstation speaker.
53
According to SFO ATCT personnel interviewed after the incident, the decision to combine
positions to a single controller was made by the controllers on duty based on the anticipated
traffic/workload and weather.
54
The SFO acting air traffic manager indicated that SFO traffic
generally begins to lessen after 0000 and tapers off significantly after 0100.
50
Both controllers who were on duty during the midnight shift were qualified as controllers-in-charge. The
controller who handled the incident flight was designated as the controller-in-charge for that shift. The SFO acting air
traffic manager stated, during a postincident interview, that two controllers-in-charge were normally staffed for the
midnight shift.
51
According to information that the controller provided during a postincident interview, he received 8 hours of
sleep on the night of July 6 through 7.
52
FAA Order JO 7210.3Z, Facility Operation and Administration, stated that “breaks to recuperate are provided
to enable employees to engage in activities necessary to rejuvenate themselves in order to effectively manage fatigue.”
(FAA Order JO 7210.3Z, which was in effect at the time of the incident, was replaced by JO 7210.3AA on October 12,
2017.) SFO ATCT personnel indicated that recuperative breaks during the midnight shift were longer than the breaks
that were normally provided during other shifts.
53
The NCT and SFO ATCT letter of agreement, titled “Coordination and Control Procedures,” stated that “each
facility must advise when going to a single person midnight operation,” but the SFO ATCT did not provide that
notification to NCT on the night of the incident. The NTSB could not determine, from the available evidence, whether
this situation was a recurring issue at the ATCT or occurred only on the night of the incident. NCT was not using
single-person operations during the time surrounding the incident.
54
The two controllers assigned to the midnight shift evaluated the pending traffic on the flight schedule monitor,
the depicted traffic in the national airspace system, and the expanded radar view of traffic within 40 miles of SFO and
decided that it was safe to combine all positions. Also, NCT had provided the ATCT with the authority to automatically
release IFR departures from SFO, which indicated a less complex traffic situation. The controller who took the
recuperative break stated that there had been a “sharp decline” in the amount of traffic displayed before the ATCT
positions were combined.

NTSB Aircraft Incident Report
19
The controller who handled the incident flight stated that traffic was “normal” before the
incident and that he was not overly busy.
55
At the time that ACA759 called to confirm whether
runway 28R was clear for landing, the controller was handling another air carrier’s tug operator,
but he checked the radar monitor and the ASSC display and rescanned runway 28R before advising
the flight crew that the runway was clear. The controller recalled that two other air carrier pilots
had contacted him just before he heard the “where is that guy going?” transmission. The controller
was unsure about who made this transmission, but he checked the ASSC display and saw that the
ACA759 data symbol no longer appeared. The controller stated that he had never seen an airplane’s
data symbol disappear when the airplane was on final approach. The controller also stated that he
was not initially concerned that the ACA759 data symbol had disappeared from the ASSC display
because he had observed the airplane from the tower cab window.
About that time, the controller heard the transmission indicating that an airplane was over
the taxiway. The controller stated that he had never seen an airplane line up with taxiway C and
that there was no indication that ACA759 was misaligned until he observed the airplane looking
“extremely strange” on short final, which was about the time when he decided to instruct the flight
crew to perform a go-around.
56
The controller stated that, about 0125 on July 8, he entered a
mandatory occurrence report into the SFO ATCT’s data analysis and reporting system; this report
was required when an airplane goes around within 0.5 mile from a landing threshold. After the
incident, the controller continued working all positions until 0300, at which time the other
controller assigned to the midnight shift returned to the tower cab.
The controller who handled the incident airplane reported that, while working
single-person operations on the night of the incident, he applied line up and wait (LUAW)
procedures for other traffic.
57
FAA Order JO 7110.65W, Air Traffic Control, which prescribes
ATC procedures, indicated that LUAW procedures should be used to position an airplane for an
imminent departure when a takeoff clearance cannot immediately be issued because of traffic.
58
Paragraph 10-3-8 of FAA Order JO 7210.3Z stated that, when applying LUAW procedures, the
“local control position must not be consolidated/combined with any other non-local control
position. For example, local control must not be consolidated/combined with the front-line
manager/controller-in-charge (CIC) position, clearance delivery, flight data, ground control, cab
coordinator, etc.” The order also stated that, during LUAW operations, “the front line
manager/CIC position should not be combined with any other position.”
During a postincident interview, the SFO acting air traffic manager stated that, if LUAW
procedures were needed to efficiently move traffic, then traffic was “too busy to combine
55
The controller also stated that he would not combine positions unless he was comfortable and had some
predictability about the tasks that he would need to perform. The controller further stated that, if the traffic had become
too busy or complex, he would have asked the other on-duty controller to return to the tower cab to assist.
56
The distance and angle (parallax) of the tower cab relative to the approach end of runway 28R and taxiway C
would have made it difficult for the controller to discern that the airplane was aligned with the taxiway instead of the
runway. Parallax is the change in apparent position due to the viewing angle.
57
During a postincident interview, the controller stated, “when aircraft were on a 5-mile final and compressing
[the distance between two aircraft was decreasing], it was hard to fit in a departure from runway 1, without using
LUAW.”
58
FAA Order JO 7110.65W, which was in effect at the time of the incident, was replaced by JO 7110.65X on
September 12, 2017.

NTSB Aircraft Incident Report
20
positions.” The SFO acting air traffic manager also stated that, after the incident, ATCT
management issued guidance indicating that the ground control and local control positions could
not be combined before 0015.
59
In addition, the SFO acting air traffic manager stated that ATCT
management had been reemphasizing the correct application of LUAW procedures.
1.4.2 Air Traffic Control Tower Equipment
The SFO ATCT was equipped with an ASSC system, which was one of three types of
airport surface detection equipment (ASDE) systems in the national airspace system. FAA Order
JO 7110.65W described the use and purpose of ASDE as follows:
Surveillance equipment specifically designed to detect aircraft, vehicular traffic,
and other objects, on the surface of an airport, and to present the image on a tower
display. Used to augment visual observation by tower personnel of aircraft and/or
vehicular movements on runways and taxiways.
Also, the order indicated that the ASSC system used surface movement radar, multilateration, and
the Automatic Dependent Surveillance-Broadcast system.
60
According to FAA Order JO 7110.65W, the ASSC system included a safety logic system
software enhancement that “predicts the path of aircraft landing and/or departing, and/or vehicular
movements on runways.” The order stated that “visual and aural alarms are activated when the
safety logic projects a potential collision.” Specifically, the system was designed to provide an
alert for “an actual situation involving two real safety logic tracks (aircraft/aircraft, aircraft/vehicle,
or aircraft/other tangible object) that safety logic has predicted will result in an imminent
collision.” The order also stated that the system could generate false and nuisance alerts and could
result in an “Invalid Non-Alert,” which involves “a situation in which the safety logic software did
not issue an alert when an alert was required, based upon the design specifications.”
According to the FAA, at the time of the incident, the ASSC system was available at SFO
and Cleveland Hopkins International Airport, Cleveland, Ohio (FAA 2018a).
61
The ASSC display
in the SFO ATCT presented aircraft and vehicle positions over a map of the airport’s runways,
taxiways, and approach corridors. The ASSC display included a two-dimensional presentation of
59
(a) At the time of the incident, the SFO ATCT’s standard operating procedures described staffing requirements
between 0630 and 2200 but did not provide such requirements between 2200 and 0630 the next day. (b) In June 2018,
the NTSB asked the SFO ATCT when the 0015 time became effective and what factors were used to determine this
time. The SFO ATCT operations manager responded that the 0015 time became effective on July 8, 2017 (the day
after the incident) and that normal traffic patterns, runway closures, administrative duties, and fatigue guidance were
considered in determining the 0015 time.
60
According to the order, the other two ASDE systems were ASDE-3, a surface movement radar, and ASDE-X,
which used an X-band surface movement radar, multilateration, and the Automatic Dependent Surveillance-Broadcast
system. The three ASDE systems functioned similarly, but the ASSC had some capabilities that the other two ASDE
systems did not have, including the ability to display extended runway centerlines and expand the capture box (block
of airspace) area.
61
According to the FAA, six additional airports were scheduled to receive the ASSC system during the next few
years.
NTSB Aircraft Incident Report
21
the runway centerlines, which extended out to about 2.5 nm. Figure 5 shows the ASSC display at
2356:21 on the night of the incident.
Source: FAA.
Figure 5. ASSC display at SFO.
Note: (a) The top of the figure shows the extended runway centerlines for runway 28R and 28L, and the bottom of the
figure shows the airport movement areas. (b) The NTSB added labels to the figure to emphasize pertinent information.
The SFO ATCT controller who was taking a recuperative break at the time of the incident
stated that the ASSC system assisted ground controllers in identifying airplanes and their locations
and preventing runway incursions. He also stated that local controllers used the system as an “extra
set of eyes” to assist with scanning and situational awareness. This controller also stated that the
ASSC system provided airplane location information starting about the time that an airplane was
on a 2-mile final approach. Another SFO ATCT controller stated that the ASSC system could be
programmed to display runway and taxiway closures.
In February 2018, the FAA conducted tests at Seattle-Tacoma International Airport (SEA),
Seattle, Washington, to determine if the ASDE-X system at the airport could detect and predict
taxiway landings with only a negligible number of nuisance or false alarms.
62
NTSB staff observed
the tests and participated in the discussion of the test results.
62
On December 19, 2015, a Boeing 737 airplane operated by Alaska Airlines landed on a taxiway instead of the
intended runway at SEA. The crew and passengers were not injured, and the airplane was not damaged. The incident
occurred during daytime VMC. For more information about this incident, see NTSB incident number DCA16IA036
.

NTSB Aircraft Incident Report
22
For the tests, the system was configured to apply the same parameters that are used to
predict a landing on a closed runway.
63
The tests included four different taxiway landing scenarios
(one of which was similar to the circumstances of the SFO incident), and an FAA flight check
airplane flew several approaches for each scenario. The tests showed that the ASDE-X system
predicted the potential taxiway landing and provided an alarm when the airplane was within
20 seconds or 3,000 ft of landing. The ASDE-X alarm occurred with enough time for ATC
personnel to respond. No false alarms occurred during any of the approaches and taxiway landing
scenarios, including those involving parallel taxiway B, which is located 407 ft to the left of
runway 16L (centerline to centerline). According to information that the FAA provided to the
NTSB on September 13, 2018, a software enhancement, the taxiway arrival prediction capability,
was implemented at SEA in May 2018, and the FAA has a schedule to evaluate the remaining
ASDE-X-equipped airports and implement the software enhancement, where feasible, by the end
of fiscal year 2020.
1.5 Tests and Research
1.5.1 Airplane Performance Study
The NTSB conducted an airplane performance study for this incident to determine the
lowest altitude over the taxiway that ACA759 reached before the initiation of the go-around and
the estimated distance between ACA759 and the second airplane on taxiway C (PAL115, which
was below ACA759 when it reached its lowest altitude). To conduct the study, the NTSB used
FDR data; radar data from the airport surveillance radar-9 at Metropolitan Oakland International
Airport, Oakland, California; and video from a security camera at an SFO terminal.
64
The security video showed ACA759 on final approach to the airport, as shown in figure 6.
The reflection of the airplane’s lights could be seen on the water in San Francisco Bay. Three of
the four airplanes on taxiway C (UAL1, PAL115, and UAL863) are visible in the figure.
63
All of the ASDE systems could be configured to predict a potential landing on a closed runway and provide
alerts if this hazard was detected.
64
The radar, which was about 10 nm from the incident location, updated data every 4.5 seconds.

NTSB Aircraft Incident Report
23
Source: SFO.
Figure 6. ACA759 on final approach to SFO.
The security video also showed ACA759 passing over the airport seawall and then passing
over UAL1 on taxiway C, as shown in figure 7. About this time, the PAL115 flight crew turned
on that airplane’s landing lights, which illuminated the taxiway between PAL115 and UAL1 as
well as the tail and side of the UAL1 airplane. In addition, the security video showed the fuselage
of PAL115, which was illuminated by the ACA759 landing lights, and ACA759 descending to its
lowest altitude as the airplane passed over PAL115. At that point, the attitude of the ACA759
airplane changed from nose down to nose up, as shown in figure 8. Subsequent frames of the
security video showed ACA759 gaining altitude over the taxiway and passing over UAL863 and
UAL1118. (UAL863 is shown in figures 7 and 8, but UAL1118 is not shown in those figures).
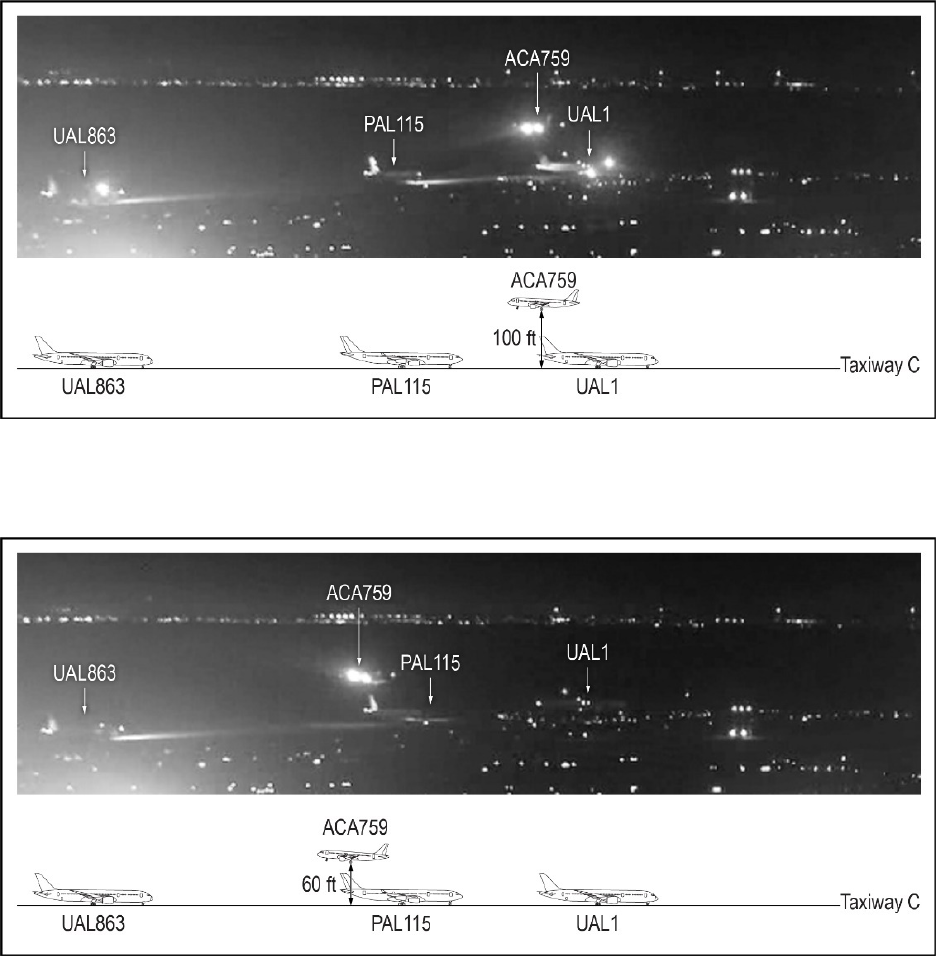
NTSB Aircraft Incident Report
24
Source for top image: SFO.
Figure 7. ACA759 passing over UAL1 (top) and relative locations of airplanes (bottom).
Source for top image: SFO.
Figure 8. ACA759 passing over PAL115 (top) and relative locations of airplanes (bottom).
Note: The PAL115 airplane, an A340, has a reported height of 55 ft. Although ACA759’s radio altimeter recorded the
height above the ground of the bottom of the landing gear to be 60 ft, the security video showed more distance between
the airplanes than the radio altimeter measurement. Specifically, the security video showed that the separation distance
between the ACA759 fuselage and the PAL115 vertical stabilizer was 13.5 ft, as explained further in this report section.
The performance study considered the incident airplane’s pressure altitude and radio
altitude, which the FDR recorded, when determining altitude points. Pressure altitude was used for
altitudes that were higher than 2,000 ft. Radio altitude—the height of the airplane above the ground

NTSB Aircraft Incident Report
25
directly below—was used for altitudes that were 2,000 ft and lower.
65
The adjusted radio altitude
reflected the bottom of the airplane’s landing gear above the ground; the landing gear extended
5 ft below the airplane’s fuselage.
The lowest adjusted radio altitude, which occurred when ACA759 passed over PAL115,
was determined to be 60 ft, which was the height of the bottom of the landing gear above the
ground. To confirm this altitude, the NTSB examined the image from the security camera video
that showed ACA759 passing over PAL115 (figure 8). In that image, the vertical stabilizer of the
PAL115 airplane (an A340) was well illuminated. The NTSB used known dimensions of an A340
vertical stabilizer to scale the image, measured the closest point between the two airplanes, and
determined that measurement to be 13.5 ft. Because the security camera image of the airplanes
was relatively small and pixilated, this measurement was estimated to be between 10 and 20 ft to
account for the inherent uncertainty. In addition, this measurement assumed that ACA759 was
directly above PAL115; the lateral separation could not be determined from the image of ACA759
passing over PAL115. The A340 airplane (including the vertical stabilizer) was reported to be 55 ft
tall, so the altitude of the ACA759 fuselage as it passed over PAL115 would have been between
65 and 75 ft, which was consistent with the 60-ft adjusted radio altitude plus the 5-ft distance
between the bottom of the landing gear and the bottom of the fuselage.
The airplane performance study also determined the track of ACA759 while it approached
SFO and was over taxiway C, as discussed in section 1.1 and shown in table 1.
1.5.2 Enhanced Ground Proximity Warning System Simulation
According to Honeywell, Air Canada installed Honeywell Mark V enhanced ground
proximity warning systems (EGPWS) on the company’s fleet of A320 airplanes. According to
Honeywell’s Mark V and Mark VII EGPWS Pilot’s Guide, the EGPWS incorporated several
terrain alerting and display features.
The EGPWS guide also described other features, including the runway awareness and
advisory system (RAAS) option, which provides “alerts and advisories that increase crew
situational awareness during operations on and around airports.” Another option was the
SmartLanding system, which, according to Honeywell, “provides visual and aural annunciations
that supplement flight crew awareness of…select RAAS advisories.” At the time of the incident,
65
According to Airbus, the radio altimeter should be set so that it reads 0 ft at airplane touchdown with an
estimated average pitch of 6°. After ACA759’s final touchdown on runway 28R (after the second approach and
landing), the radio altimeter recorded a value of -2 ft. For the airplane performance study, the radio altimeter
measurement was adjusted +2 ft (the approximate height of the main landing gear wheels above the ground). No
adjustments were made for the pitch of the airplane. In addition, the image of ACA759 and PAL115 when they were
at their closest point was relatively small in the video frame, so the measurements were approximations. Thus, the
altitudes derived in the study had uncertainty associated with them.

NTSB Aircraft Incident Report
26
the EGPWS installed in Air Canada’s A320-200 fleet, including the incident airplane, did not
include the RAAS or the SmartLanding system options.
66
The NTSB asked Honeywell to conduct a simulation to determine if an EGPWS with the
SmartLanding system would have alerted the incident flight crew about the potential taxiway
landing. The simulation was run using a Mark V EGPWS in Honeywell’s laboratory in Redmond,
Washington. Honeywell set the taxiway landing alert threshold at a radio altitude of 250 ft, which
was the default setting, and incorporated parameters from the incident airplane’s FDR.
67
The aural
taxiway landing alert, “Caution Taxiway, Caution Taxiway,” was designed to annunciate between
a radio altitude of 250 and 150 ft. The simulation showed that the incident flight crew would have
received the aural taxiway landing alert when the airplane was at a radio altitude of 235 ft and was
2,600 ft (0.43 nm) from the airport seawall. According to the results of the airplane performance
study, the incident airplane reached that altitude just before the tower controller confirmed that
runway 28R was clear.
The NTSB notes that Honeywell’s systems are examples of available systems designed to
augment a pilot’s positional awareness during in-flight and ground operations; Garmin also has
such a system available, and Rockwell Collins has a system in development. The three Honeywell
systems described in this section all provide the alert “approaching [runway number]” before
landing.
1.6 Organizational Information
1.6.1 Descent, Approach, and Arrival Information
Air Canada’s A319/A320/A321 Aircraft Operating Manual, volume 1, section 4, “Standard
Operating Procedures,” provided flight crews with information on preparing for the descent to the
destination airport. The manual stated that descent preparation should be completed before the top
of the descent. The manual also stated that the pilot monitoring was to “set navaids as required”
on the “RAD NAV [radio/navigation]” page (referenced with the MCDU) and “check idents
on…PFDs (ILS).” The manual further stated that the pilot flying was to review all MCDU
programming by the pilot monitoring, including entries on the radio/navigation page.
Air Canada’s A319/A320/A321 Aircraft Operating Manual, volume 2, section 22-30,
“Auto Flight – Flight Guidance,” stated that the open descent mode maintains a target speed/Mach
number with the autopilot/flight director pitch mode while autothrust (if activated) maintains idle
thrust (unless the flight crew maintains idle thrust manually). Volume 1, section 4 of the manual,
“Standard Operating Procedures,” described a selected approach (also referred to as an open
66
(a) Honeywell’s Mark V and Mark VII EGPWS Pilot’s Guide indicated that RAAS required a GPS source. At
the time of the incident, Air Canada operated 42 A320-200 airplanes, some of which were equipped with a GPS; the
incident airplane was not equipped with a GPS. A June 2018 e-mail from Air Canada to the NTSB indicated that all
of the airplanes in the company’s A320-200 fleet had been equipped with a GPS. (b) Honeywell also offered another
optional feature, the SmartRunway system, which was designed to alert flight crews to an impending taxiway landing
as well as an impending taxiway takeoff.
67
The FDR did not record true track, true heading, and vertical speed parameters, which were necessary for the
simulation, so Honeywell derived those parameters using the magnetic heading, magnetic variation, drift angle, and/or
pressure altitude that the FDR recorded.

NTSB Aircraft Incident Report
27
approach) as “Autopilot or Flight Director systems directed by pilot selected commands” and a
managed approach as “Autopilot or Flight Director systems directed by FMGS [flight management
guidance system] capabilities.”
68
The FMGS-generated information on the electronic flight
instrument system included the flight plan, the airplane’s position and lateral deviation from the
flight plan, the approach, and raw data from tuned navigational aids.
Air Canada’s Flight Operations Manual, section 8.9.10.1, “Arrival Preparation,” stated
that, before briefing the arrival and approach, a flight crew should obtain the current ATIS, review
applicable NOTAMs, and program the FMS/FMGS with the required data and cross-check the
entries with the appropriate charts. Section 8.9.10.3, “Arrival and Approach Briefing,” provided
flight crews with information on briefing the approach and arrival into an airport. The manual
stated that the purpose of the arrival and approach briefings, which the pilot flying was required to
perform for all approaches (including visual approaches), was “to enhance situational awareness
and clarify expectations.” The manual also addressed the threat briefing, indicating the following:
Beginning with the Pilot Monitoring (PM)…and ending with the Pilot Flying (PF),
each crew member should identify any relevant threats that are anticipated during
descent, arrival, approach, landing and taxi-in that pertain to their role, as well as
strategies to mitigate them.
Air Canada’s Threat Briefing Reference Card indicated that a threat briefing was expected
to be performed as part of the approach briefing. The card also indicated that the threat briefing
was to be performed by both the pilot flying and the pilot monitoring. The card included examples
of threats involving the airplane, operations, ATC, the runway, adverse weather, the operating
environment, and the flight crew.
69
“NOTAMS” was listed under the “Operations” heading,
“Lighting” was listed under the “Runway” heading, and “Alertness” was listed under the
“Flight Crew” heading.
Air Canada’s A319/A320/A321 Aircraft Operating Manual, volume 1, section 4, “Standard
Operating Procedures,” provided flight crews with guidance about crew coordination during the
approach. The manual stated the following:
The PM must maintain a high level of vigilance in monitoring aircraft position,
attitude and configuration and pay close attention to instrument indications. The PF
must monitor position through both external references and by reference to NAV
systems, including DME [distance measuring equipment] and NAV Display. Use
automation functions to the greatest extent possible. Good crew communication is
important.
Air Canada’s A319/A320/A321 Aircraft Operating Manual, volume 1, section 11,
“Approach,” provided flight crews with stabilized approach criteria for various approaches. For
68
A managed descent is also directed by the FMGS. Most of the Air Canada pilots who were interviewed after
the incident stated that they would have flown the FMS Bridge visual approach to runway 28R as a managed descent
due to the altitude restrictions and the associated increased workload. Also, the incident first officer stated that he flew
a managed descent during the flight into SFO 2 nights before the incident.
69
The threat briefing card further indicated that the threats included on the card were not “an exhaustive list of
all possible threats” and that the flight crew was responsible for briefing any additional threats that might be present.

NTSB Aircraft Incident Report
28
visual approaches, the manual provided the following criteria: “lateral tracking as close as possible
to the extended runway centerline or published inbound course” and “vertical tracking on
approximately a 3 degree glide path and using visual approach slope indicators…if available.”
70
The manual also stated that the pilot flying and the pilot monitoring should closely monitor flight
parameters and that the pilot monitoring should call out any deviation that exceeded the established
parameters. Air Canada’s Flight Operations Manual, section 8.11.9.3, “Go-Around,” stated that a
go-around should be initiated if “stable approach parameters cannot be met and maintained inside
the appropriate gates” (1,000 and 500 ft above airport elevation).
71
1.6.2 Crew Resource Management
Air Canada provided its pilots with a crew resource management (CRM) manual that
included, among other subjects, communication, situational awareness, planning,
decision-making, workload management, active monitoring, and threat and error management. A
separate document, the company’s CRM competency guide, addressed each pilot’s responsibilities
in the areas of situational awareness, decision-making and problem solving, workload
management, professional management, and active monitoring and threat and error management
procedures. In the area of situational awareness, the guide indicated that a captain was to
“recognize and effectively respond to indications of reduced situational awareness from other crew
members.” In the area of active monitoring and threat and error management procedures, the guide
indicated that the pilot monitoring was to “communicate all errors, omissions, and differences in
situational awareness and ambiguities to the PF assertively.” Also, in the area of active monitoring
and threat and error management procedures, all pilots were to “detect deviations from the desired
aircraft trajectory and take appropriate action.”
Air Canada provided CRM training during new hire, recurrent, and command upgrade
training. The incident captain reported that the training was conducted in a classroom setting with
mostly lectures and some scenarios. In 2016, Air Canada revised its CRM training to reflect a
threat and error management model. This model focused on the following four levels (from top to
bottom) of threat management:
• Proactive—the flight crew briefs and mitigates threats before they are encountered.
• Reactive—an unexpected threat has occurred that the crew must recognize and
respond to. If the crew manages the threat, then no error occurs.
• Errors and error management—the crew has mismanaged the threat, and a
procedural, communication, or handling error has occurred. If the crew traps the
error, safety margins will be maintained.
70
Postincident interviews and airplane track data suggested that the flight crew used the precision approach path
indicator located to the left of runway 28R for glidepath information. FDR data showed that, after the airplane passed
F101D (at an altitude of about 1,100 ft), the airplane’s glidepath was between 2.1° and 3.2°.
71
As discussed in section 1.1, other criteria for initiating a go-around were “landing will not be accomplished
within the touchdown zone” and “landing will not be accomplished on the runway centerline.”

NTSB Aircraft Incident Report
29
• Undesired aircraft state—a flight crew-induced aircraft state has occurred that
clearly reduces safety margins and results in a safety-compromised situation.
The captain’s and the first officer’s CRM skills were highly rated by other pilots who had
flown with them. Although a check airman expressed concern about the first officer’s situational
awareness (as indicated in section 1.2.2), the check airman described the first officer’s overall
CRM as “good.”
1.6.3 Fatigue Information
Air Canada’s Flight Operations Manual provided information regarding the development
of fatigue and fatigue management. Section 4.12.3, “Circadian Basics,” stated that humans “have
an internal circadian clock that regulates physiological and behavioural functions on a 24-hour
basis” and that “the clock coordinates daily cycles of sleep/wake, performance, physiology, mood,
and other functions.” The manual also discussed circadian disruption by stating that “the circadian
clock cannot adjust immediately when a person suddenly changes schedule (e.g., by flying into a
new time zone or changing to a new work/rest schedule).” The manual further stated that flying
into a new time zone produces “a challenge to the circadian clock” because “it can take several
days or weeks for the clock to get into step with the new local time.” In addition, the manual stated
that, between 0300 and 0500 (body clock time zone), “physiological sleepiness peaks, and virtually
all aspects of alertness and performance slow and can be reduced.”
Section 4.12.5, “Preventive Strategies,” stated that “naps can acutely improve alertness and
performance, and even short naps can provide benefits.” The manual also stated that “a nap reduces
the duration of continuous wakefulness before a work period, and can be particularly beneficial
before a period of night work, when the challenge of working through the circadian low point is
also a factor.”
Section 4.12.6, “Operational Countermeasures,” discussed strategies for pilots to
counteract fatigue while on duty. The section noted that such countermeasures, which included
controlled rest (a planned cockpit rest period to improve subsequent performance and alertness)
were “meant to temporarily enhance alertness and performance…so that operational safety and
efficiency are maintained.” Regarding controlled rest, the manual advocated the use of “strategic
naps” in appropriate circumstances and indicated that “napping is the only operational
countermeasure that addresses one of the major physiological causes of fatigue – the need for sleep
– and reverses it.”
72
1.6.4 Event Reports
Air Canada’s Flight Operations Manual, section 12.2, “Definitions, Procedures, and
Report,” stated the following: “Any aircraft accident, incident, emergency, or other safety related
event which may require investigation, monitoring or tracking shall be reported to Dispatch as
soon as possible. In addition, the flight crew should file an ASR [air safety report] when time
72
Air Canada officials stated, during postincident interviews, that the company’s controlled rest policy is
generally used by overseas flight crewmembers who do not have a relief crewmember. Air Canada requests that
crewmembers who use the controlled rest policy file a fatigue report.

NTSB Aircraft Incident Report
30
permits.”
73
(ASRs are voluntary.) The section provided examples of reportable safety events,
including unusual or abnormal aircraft handling; significant navigation errors or technical
navigation problems; breach of air regulations, ATC irregularities, or a near miss; an unstable
approach; a go-around; and any other hazard that poses a direct threat to flight safety.
Chapter 3 of the manual, “Safety Management System,” section 2.5.1, stated that an ASR
is “an electronic or paper medium through which employees are able to identify hazards, incidents,
and accidents which impact the operational safety of Air Canada.” The section also stated that
ASRs are “de-identified and accessible by all levels of management who are required to regularly
review, provide feedback, and monitor the progress of analysis and investigations.”
During postincident interviews, the first officer stated that he and the captain met about
1100 on the morning after the incident to discuss the facts of the incident for the ASR, and the
captain stated that he contacted company flight dispatch later that day to report the event.
74
Air
Canada records showed that the captain reported the event to dispatch about 1608 (1908 EDT) on
July 8. The dispatcher who spoke with the captain stated that he reported that the airplane was
lined up with the wrong runway and that a go-around ensued.
75
The dispatcher also stated that the
captain’s report sounded “innocuous” and that, because of the late notification (16 hours after the
incident), he did not think that the event was serious.
The captain stated that he also spoke with the duty pilot to report that he had aligned the
airplane with a taxiway and performed a go-around.
76
The captain indicated that the duty pilot
asked him whether the localizer was tuned, and the captain replied that it was not tuned for the
first approach but was tuned for the second approach. According to Air Canada’s vice president of
safety, after the flight crew notified the duty pilot of the incident, the senior director of line
operations determined that the flight crew would be allowed to operate the flight from SFO to
YYZ (using a different airplane than the incident airplane) and then “would be held out of service”
after arriving at YYZ later that day. Air Canada’s director of corporate safety, investigations, and
research stated that the incident airplane had flown about 40 hours before Air Canada senior
officials became aware of the severity of the incident and realized that data from the airplane
needed to be retrieved.
77
Air Canada’s safety department was not consulted on the decision to keep
73
(a) Air Canada’s Flight Operations Manual, section 8.16, “Post Flight,” stated that flight crews should brief
company dispatch after a flight about any “significant operational factors.” (b) At the time of the incident, Air Canada
did not define “as soon as possible” regarding the pilot’s responsibility to report events to dispatch. In a May 2018
revision to its Flight Operations Manual, Air Canada defined “as soon as possible” as “to accomplish promptly or as
soon as time permits.” This and other postincident actions taken by Air Canada are discussed in appendix B.
74
The captain stated that he did not report the incident to company dispatch shortly after it occurred because he
was “very tired” and it was “very late.”
75
The NTSB listened to a recording of the captain’s call to dispatch and confirmed that the captain indicated that
he aligned the airplane with the “wrong runway.”
76
Air Canada’s Flight Operations Manual, chapter 3, “Organizational Structure, Publications, and
Documentation,” stated that the duty pilot was an Air Canada flight operations manager who was responsible “for all
operational and administration decisions during times when other managers are not available.” The duty pilot acted
on behalf of Air Canada flight operations senior management.
77
FDR data showed that the incident airplane departed SFO at 0747 (1047 EDT) on July 8 and arrived at Pierre
Elliott Trudeau International Airport, Montreal, Canada, the same day at 1245 (1545 EDT). Because the airplane
continued to fly after the incident occurred, CVR data from the incident flight were overwritten, and the FDR recorded
more than 41 hours of data during eight flights after the incident flight.

NTSB Aircraft Incident Report
31
the incident airplane in service and have the flight crew continue with the planned flight to YYZ,
even though the safety department was generally included on such decisions.
78
During a postincident interview, the captain stated that the duty pilot asked him to file an
ASR. The captain indicated that he had filed an ASR on July 8, but Air Canada’s director of
corporate safety, investigations, and research stated that no safety report was on file when he
learned about the event through an e-mail from the Transportation Safety Board of Canada (TSB)
about 2200 EDT on July 9.
79
(This director stated that the ASR had been “sitting in the system”
and was received on either July 10 or 11. The director further stated that company tablets were
used to send ASRs and that the reports could only be transmitted if a tablet was connected to
Wi-Fi.)
The Air Canada A320 assistant chief pilot stated, during a postincident interview, that she
and other Air Canada officials met with the incident flight crew on July 10. According to the A320
assistant chief pilot, the flight crewmembers stated that they performed a go-around at an altitude
of about 400 feet and that they did not realize that the airplane was aligned with a taxiway until
“very late in the approach.” She also stated that the crewmembers were then told that ACA759 had
overflown airplanes on a taxiway and that the crewmembers’ responses were “shock” and
“surprise.”
In addition, the SFO acting air traffic manager reported that he and other ATCT personnel
interviewed the incident captain at 1140 on July 8. During that conversation (which was not
recorded), the acting air traffic manager notified the captain of the possible pilot deviation.
According to FAA Order JO 7210.632, Air Traffic Organization Occurrence Reporting, this
notification is provided when an “employee providing air traffic services determines that pilot
actions affected the safety of operations.” The order also indicated that this notification was to be
part of the air traffic mandatory occurrence report and that the flight crew should be notified “as
soon as operationally practical.”
80
1.6.5 Plan Continuation and Expectation Bias Training
On April 1, 2017, Air Canada implemented part of its training on plan continuation and
expectation bias, which was presented to company pilots during annual recurrent training.
81
This
training comprised an 8-minute video, titled “Understanding Gut Feel.” The video explained that
a gut feeling was “a sense of knowing things before we can consciously know them, or
communicate them, or even explain them.” The video also explained that a gut feeling signaled
that “something about this moment is different or strange, something has changed, and this
78
The NTSB could not determine, on the basis of the available evidence, why Air Canada’s safety department
was not consulted on these decisions, but the company’s flight operations department had the authority to make such
decisions without contacting the safety department.
79
The NTSB learned about this incident from the FAA on July 9 at 1630 EDT (see appendix A) and notified the
TSB about the incident at 1840 EDT the same day.
80
The FAA order further indicated that this notification was “intended to provide the involved flight crew with
an opportunity to make note of the occurrence and collect their thoughts for future coordination with Flight Standards
regarding enforcement actions or operator training.”
81
Air Canada developed this training after collaborating with a human factors contractor (who was hired a few
years before the incident) to help improve the company’s performance.

NTSB Aircraft Incident Report
32
something, yet to be discovered, poses a potential threat.” The video further explained that this
“signaling usually lasts for only 3 to 4 seconds before we either check it out or talk ourselves out
of what it is trying to tell us,” which “complicates our ability to translate the messages from the
gut.”
The video presented a basic strategy for listening to gut feelings when evaluating a
situation, as expressed by the acronym “LIVE”: listen (to signals), investigate (what has changed
or is different), validate (test and confirm a theory about what is different), and express
(communicate the concern to others). The video added that, once a person begins listening to gut
feelings, that person will become “much more aware and connected” to a working environment.
The incident flight crewmembers had not received this training at the time of the incident
because both had completed their most recent training (during the 2016/2017 training cycle) before
the video became available (as part of the 2017/2018 training cycle). Air Canada indicated that the
incident flight crewmembers would receive the training during their next annual recurrent training.
As part of its plan continuation and expectation bias training, Air Canada planned to
introduce a 49-slide PowerPoint presentation during the 2018/2019 training cycle to (1) help
company pilots understand why experienced professional pilots make errors and (2) examine
mitigation strategies to overcome plan continuation and expectation bias. The NTSB’s review of
the planned presentation found that it defined plan continuation bias as “unconscious cognitive
bias to continue [an] original plan in spite of changing conditions” and expectation bias as “when
someone expects one situation, she or he is less likely to notice cues indicating that the situation
is not quite what it seems.” The slides presented two case studies, one in which a flight crew was
affected by plan continuation bias, which led to a loss of situational awareness, and one in which
a flight crew was affected by expectation bias, which led to crew confusion. The slides also
presented countermeasures (which were company CRM competencies) to prevent plan
continuation and expectation bias.
1.6.6 Flight Information
Air Canada’s FMS Bridge visual approach to runway 28R, the NOTAM information that
Air Canada provided in the ACA759 flight release to notify the flight crew about the runway 28L
closure, and the display of the ATIS information transmitted to the flight crew about 2321 are
shown in figures 9 through 11, respectively.
82
The NTSB added a highlighted box with a dashed
82
The first officer stated that Air Canada had recently transitioned from paper flight releases to digital flight
releases that were accessed on company tablets. The first officer also stated that he would circle or highlight important
items on paper flight releases but that the company tablets in use at the time of the incident did not have that capability.
(The NTSB notes that the presentation of approach chart information was the same in the paper and electronic
versions.) After the incident, Air Canada developed a means for its flight crews to highlight areas or make notes on
digital flight releases.
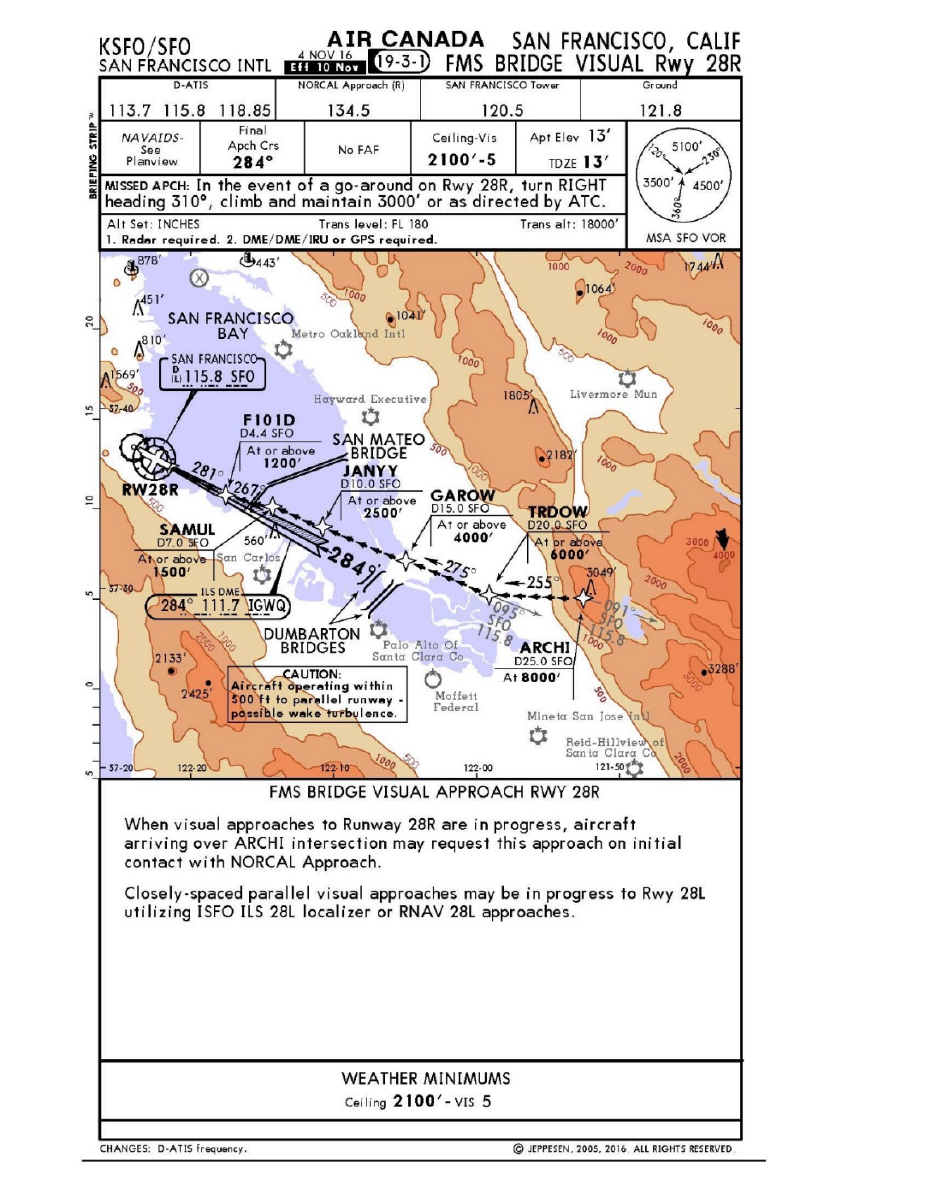
NTSB Aircraft Incident Report
33
outline to each of these figures to emphasize information related to the circumstances of this
incident.
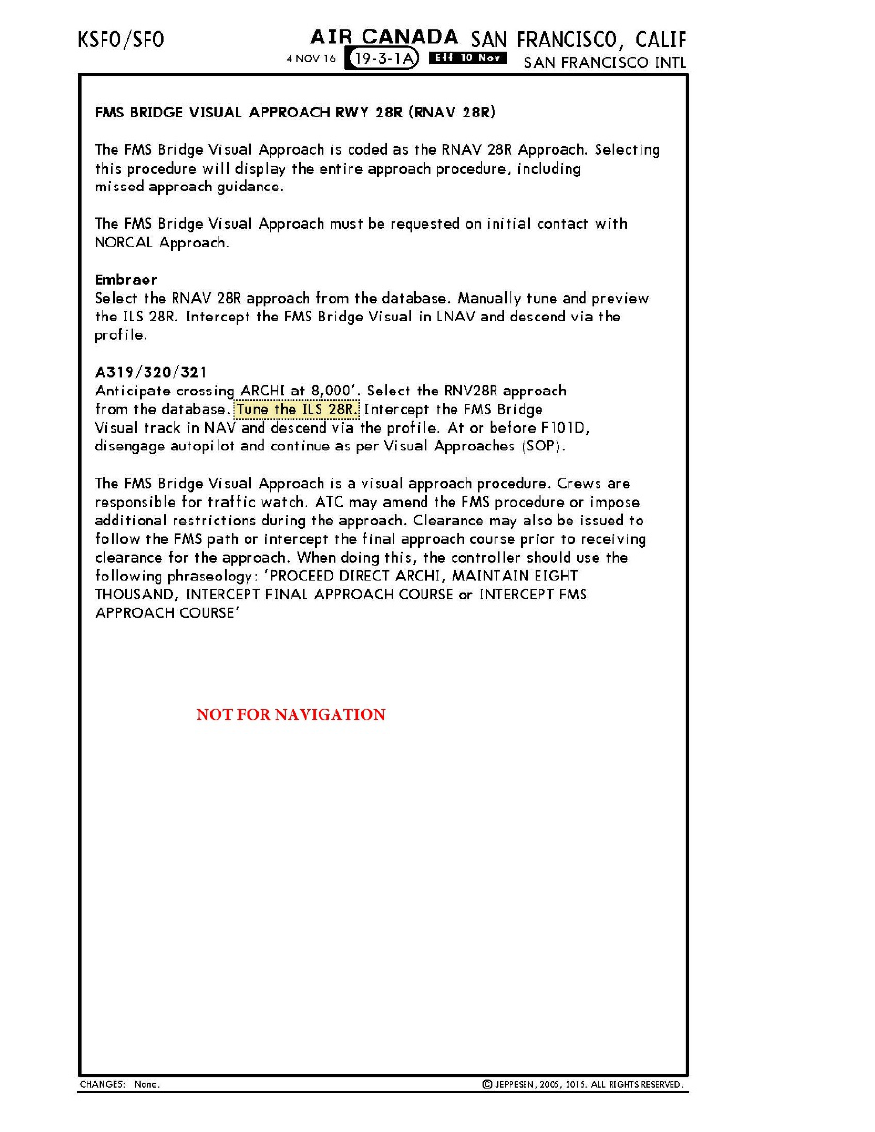
NTSB Aircraft Incident Report
34
Source: Air Canada.
Figure 9. Approach procedure (two pages).
Note: The NTSB added the highlighted box with a dashed outline (on the second page of the approach procedure) for
emphasis. The approach chart is 8.5 inches long and 5.5 inches wide.
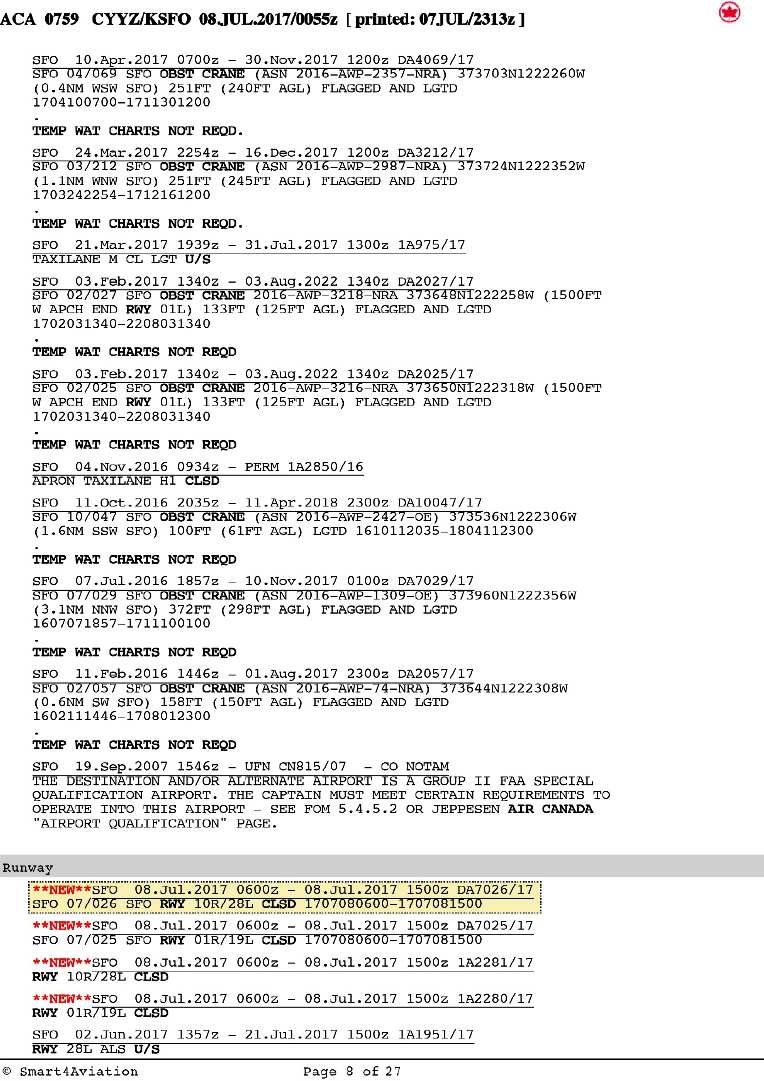
NTSB Aircraft Incident Report
35
Source: Air Canada.
Figure 10. NOTAM showing runway 28L closure.
Note: (a) The NTSB added the highlighted box with a dashed outline for emphasis. (b) The information on this page of
the flight release appeared under the gray highlighted heading “DESTINATION” on the previous page of the flight
release. (c) The highlighted NOTAM was issued by the FAA; the third “NEW” NOTAM, which contains the same
information as the FAA (domestic) NOTAM, was issued by the International Civil Aviation Organization. (d) Paper flight
release information is 11 inches long and 8 inches wide.
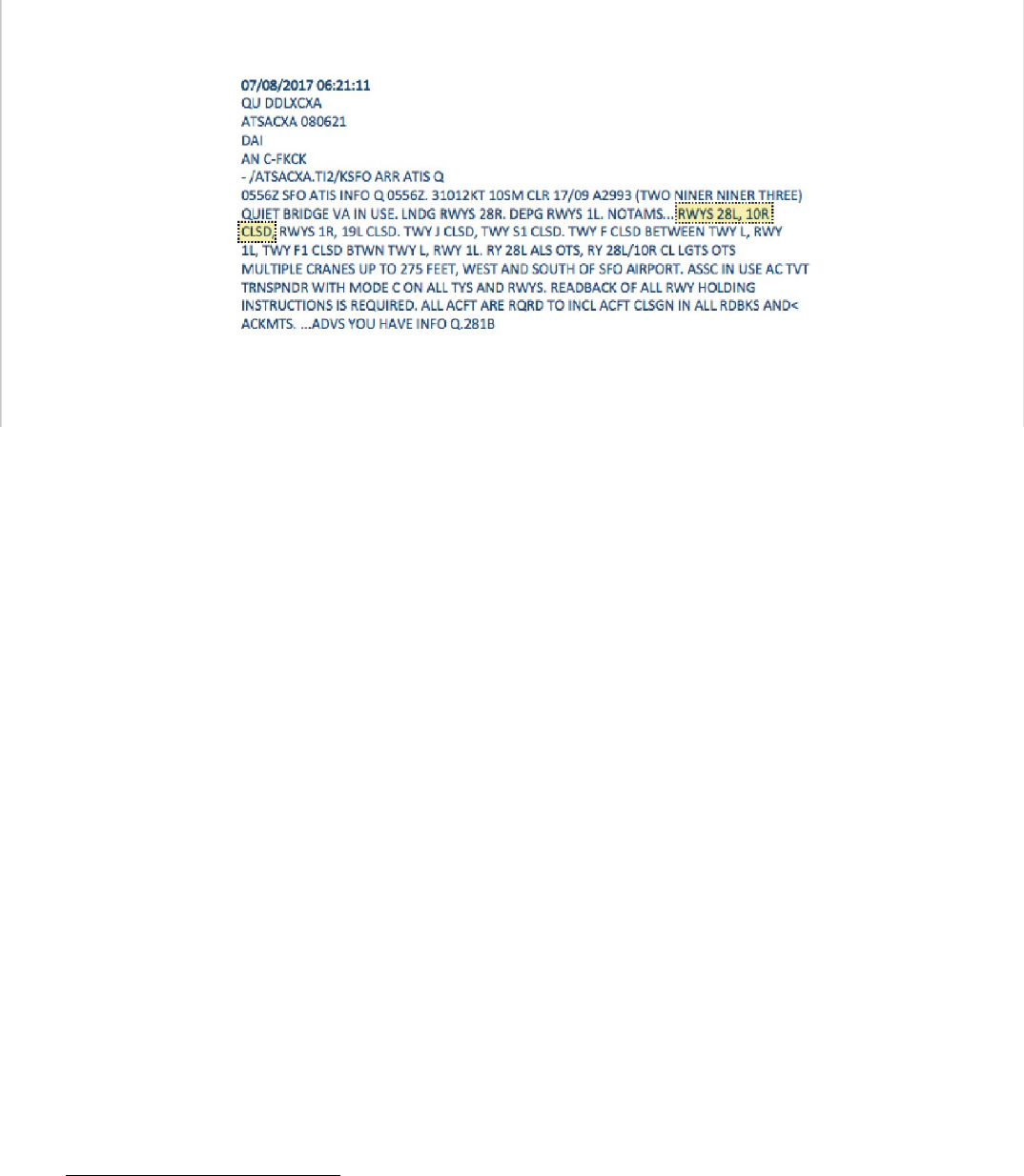
NTSB Aircraft Incident Report
36
Figure 11. ATIS information Quebec.
Note: (a) The NTSB added the highlighted box with a dashed outline for emphasis. (b) This display of ATIS information,
which was based on the raw text provided by Air Canada, represents what the flight crew would have seen on the
ACARS screen. Nonpertinent items from the raw text, such as coding at the end of each line, have been deleted. The
docket for this incident contains the raw ATIS information text. (c) ACARS information is printed on a paper roll that is
4.25 inches wide. The length varies according to the information to be printed.
1.7 Additional Information
1.7.1 Wrong Surface Landings Video
In August 2018, the FAA announced its new video highlighting wrong surface landings
and provided pertinent data as part of the announcement (FAA 2018b). The FAA’s data showed
that 85% of wrong surface landings involved general aviation aircraft (with the remainder
involving commercial aircraft). The data also showed that parallel runways accounted for 75% of
wrong surface landings. In addition, the video (dated July 25, 2018) indicated that 85% of wrong
surface landings occurred at level 9 or lower ATCT facilities.
83
1.7.2 Safety Alert for Operators
On August 18, 2017, the FAA issued Safety Alert for Operators (SAFO) 17010, “Incorrect
Airport Surface Approaches and Landings,” to provide “some best practices for approaching and
landing on the correct airport surface.” The best practices described in the SAFO included
83
Small ATCT facilities are classified as levels 4 through 6, and medium ATCT facilities are classified as levels 7
through 9. The SFO ATCT was considered to be a level 10 facility.
NTSB Aircraft Incident Report
37
• performing a stabilized approach, which “is critical to pilots and flightcrews for
maintaining situational awareness of the external environment”;
• using technology, including ILS and RNAV published approaches or FMS RNAV aids “to
support pilot and flightcrew decisions”;
• employing CRM, which is “imperative because it leverages the skills of all
crew-members…and delineates job functions and the expectation of support”;
• using available resources, which include reviewing airport lighting, reviewing and
discussing NOTAMs, and monitoring ATIS information; and
• being ready to go around, including understanding the reasons why a go-around might be
warranted and, if necessary, taking that action “early, particularly during a time of
confusion.”
The SAFO indicated that the SFO incident highlighted the importance of these best
practices. In the SAFO, the FAA strongly urged directors of operations, directors of safety,
directors of training, and chief pilots to collaborate to
• emphasize existing procedures to ensure approaches to and landings on the correct airport
surface,
• provide information to flight crewmembers about recent incorrect surface landing events
and the importance of proactively reducing that hazard,
• ensure that all training refers to best practices that support approaches to and landings on
the approved runway, and
• emphasize the need for crew rest and vigilance when a work schedule “takes a crewmember
outside of his or her normal day.”
1.7.3 Canadian Fatigue Regulations
Canada’s flight and duty time and rest requirements have been in effect since 1996.
Transport Canada’s “Guidance Material Concerning Flight Time and Flight Duty Time
Limitations and Rest Periods,” indicated the following about pilots on reserve duty:
NTSB Aircraft Incident Report
38
When a flight crew member is on reserve, an air operator must provide the flight
crew member with the opportunity to obtain at least 8 consecutive hours [of] sleep
in any 24 hours by one of the 3 methods indicated in the standard. When that flight
crew member is contacted and required to report for duty during the period of
reserve duty, the flight crew member is no longer considered to be on reserve but
on duty…. This means that at anytime during the reserve period, a flight crew
member can be required to start a 14 hour duty period…. A flight crew member
therefore must remain rested while on reserve such that they are able to cope with
a full duty day if called.
Air Canada Pilots Association and Safer Skies, which comprises five unions in Canada,
have been advocating for stricter rest requirements and flight time limitations to address pilot
fatigue, including fatigue in reserve duty pilots. In 2010, the Canadian Aviation Regulatory
Advisory Council Working Group began an effort to update Canada’s regulations relating to
fatigue (Canadian Aviation Regulations 700.16, “Flight Duty Time Limitations and Rest
Periods.”) In 2014, Transport Canada released a draft of proposed new regulations and, in 2017,
revised the draft regulations, but no changes to regulations relating to fatigue have been
implemented.
NTSB Aircraft Incident Report
39
2. Analysis
2.1 Introduction
This incident occurred when ACA759 overflew four air carrier airplanes on a taxiway at a
low altitude. ACA759 had been cleared to land on runway 28R at SFO, but the flight crew aligned
the airplane with parallel taxiway C instead. The flight crew initiated a go-around, which avoided
a collision between ACA759 and one or more of the airplanes on the taxiway. None of the
crewmembers and passengers aboard the airplanes were injured, and none of the airplanes involved
in this event were damaged. ACA759 was operated by Air Canada under IFR and the provisions
of 14 CFR Part 129.
The following analysis discusses the incident sequence (section 2.2) and evaluates the
following:
• reasons for the flight crew’s surface alignment error, including the roles of expectation bias
and fatigue (section 2.3);
• the reporting of the incident (section 2.4);
• ATC issues, including frequency congestion and the technology available to SFO
controllers at the time of the incident (section 2.5); and
• the effectiveness of runway closure markers currently in use in the national airspace system
(section 2.6).
After completing a comprehensive review of the circumstances that led to this incident, the
investigation established that the following factors did not contribute to the cause of the incident:
Flight crew qualifications. The flight crew was properly certificated and qualified in
accordance with Canadian regulations, Air Canada requirements, and 14 CFR Part 129.
Flight crew medical conditions. The flight crew held valid and current Canadian medical
certificates. The captain and the first officer reported no medications, medical conditions, or sleep
disorders during their required medical examinations and during postincident interviews.
Airplane mechanical conditions. The airplane was properly certificated, equipped, and
maintained in accordance with Canadian regulations and 14 CFR Part 129. No evidence indicated
any structural, engine, or system failures.
Airport lighting. Runway 28R (the intended landing runway for the flight) and parallel
taxiway C at SFO met the requirements for lighting in 14 CFR Part 139. The runway 28R approach
lights were on as the incident airplane approached SFO. Title 14 CFR 139.311 required taxiways
to have one of four types of lighting systems, one of which was centerline lights, which were
present and illuminated on taxiway C. The runway and taxiway centerline lights were set at step 1
(out of 5), which was appropriate for the weather conditions on the night of the incident.

NTSB Aircraft Incident Report
40
Thus, the NTSB concludes that none of the following were factors in this incident:
(1) flight crew qualifications, which were in accordance with Canadian and US regulations;
(2) flight crew medical conditions; (3) airplane mechanical conditions; and (4) airport lighting,
which met US regulations.
2.2 Incident Sequence
2.2.1 Notification of Runway 28L Status
SFO runway 28L was scheduled to close at 2300 on the night of the incident due to
construction, and a NOTAM in the flight release for ACA759 provided information about the
closure. The captain stated that he and the first officer discussed the runway 28L closure while at
the departure gate but that they did not place much emphasis on this information because the
captain thought that the flight would land before the runway would be closed.
84
(The NTSB notes
that the flight was originally scheduled to land 3 minutes after the runway 28L closure.) However,
the airplane pushed back from the gate 30 minutes late due to the delayed arrival at YYZ of the
airplane to be used for the flight and took off about 49 minutes later than the scheduled takeoff
time. Even though the flight crewmembers knew, during their preflight preparations, about
ACA759’s delayed departure, no evidence indicated that the crewmembers reconsidered the
importance of the NOTAM information at that time or as the airplane approached SFO. For
example, as part of the approach briefing, the flight crew was required to perform a threat briefing,
but none of the threats that the pilots reportedly briefed related to the runway 28L closure.
85
Air Canada’s standard operating procedures for preparing for an arrival into an airport
indicated that the flight crew was, among other things, to obtain the current ATIS and review
applicable NOTAMs. ACARS data showed that the flight crew requested ATIS information, and
the ACARS message displaying ATIS information Quebec was sent to the airplane about 2321,
which was several minutes before the airplane began its descent from cruise altitude; at that time,
the crew’s workload would likely have been lighter compared with later phases of flight. The ATIS
information included a NOTAM indicating that runway 28L was closed, but neither flight
crewmember recalled seeing this information. Section 2.3.2 discusses the effect of the runway 28L
closure on the flight crew’s ability to identify the intended landing surface.
2.2.2 Preparations for the Descent
Air Canada standard operating procedures stated that descent preparation should be
completed before the top of the descent and listed the tasks that needed to be completed. The pilot
monitoring (in this case, the first officer) was to use the MCDU to reference the radio/navigation
page and set navigational aids into the FMC and then check that the ILS identifier shown on the
84
The captain provided this account during his second postincident interview with the NTSB. This information
differed from the account that he provided, and the account that the first officer provided, during their first postincident
interviews with the NTSB (see section 1.1).
85
As previously stated, Air Canada’s Threat Briefing Reference Card indicated that NOTAM information was
one of the threats expected to be included in a threat briefing.

NTSB Aircraft Incident Report
41
PFDs was correct.
86
The pilot flying (in this case, the captain) was to review the approach
programming in the MCDU and complete an approach briefing, which included verifying that the
primary approach aid (ILS) identifier and frequency were properly set.
ATIS information Quebec indicated that the Quiet Bridge visual approach was in use and
that arriving airplanes would be landing on runway 28R. The flight crew used Air Canada’s FMS
Bridge visual approach procedure, which was based on the Quiet Bridge visual approach
procedure, for the approach to runway 28R. Air Canada’s FMS Bridge visual approach chart
consisted of two pages. The first page showed the approach procedure and included the ILS
frequency for runway 28R in the plan view. The second page of the approach chart was in text
format and indicated that Airbus A319/A320/A321 pilots should tune the ILS for runway 28R,
which would provide flight crews with backup lateral guidance (via the localizer aligned with the
runway heading) during the approach. This lateral guidance would supplement the visual approach
procedures.
The first officer stated that, when he set up the approach in the FMC, he missed the step in
the procedure to manually tune the ILS frequency, and FDR data showed that no ILS frequency
had been entered for the approach. According to Air Canada personnel, the FMS Bridge visual
approach was the only approach in the company’s Airbus A320 database that required manual
tuning of an ILS frequency, which might have contributed to the first officer’s failure to input the
frequency (as discussed below). However, the first officer’s error should have been caught by the
captain as part of his verification of the approach setup during the approach briefing. If cockpit
voice recorder (CVR) information had been available for this incident (as discussed further in
section 2.4), the NTSB might have been better able to determine whether distraction, workload,
and/or other factors contributed to the first officer’s failure to manually tune the ILS frequency
and the captain’s failure to verify that the ILS frequency was tuned. The NTSB concludes that the
first officer did not comply with Air Canada’s procedures to tune the ILS frequency for the visual
approach, and the captain did not comply with company procedures to verify the ILS frequency
and identifier for the approach, so the crewmembers could not take advantage of the ILS’s lateral
guidance capability to help ensure proper surface alignment.
The flight crew of DAL521, which preceded the incident airplane to SFO, was also flying
the FMS Bridge visual approach to runway 28R. The DAL521 airplane landed on runway 28R
without incident (despite confusion regarding the identification of the runway surface, as discussed
in section 1.1.1) because the flight crew used LNAV guidance to align with the runway. The
DAL521 captain confirmed that the airplane was aligned with runway 28R as he visually acquired
the painted “28R” on the runway surface when the airplane was at an altitude of about 300 ft. The
DAL521 captain stated, during a postincident interview, that the runway 28R and taxiway C
surfaces could have been confused if the approach was not backed up with lateral guidance.
The incident captain’s failure to recognize that the ILS frequency had not been manually
tuned suggests insufficient preparation for the approach.
87
The first officer might have missed the
86
One of the incident flight crewmembers would have had to select the “LS” buttons on the glareshield for ILS
information to appear on the PFDs.
87
The captain’s request for the first officer to set the runway heading, as discussed in section 2.2.3, also suggests
insufficient preparation for the approach.

NTSB Aircraft Incident Report
42
step to manually tune the ILS frequency because Air Canada flight crews were not required to take
this action for any approach other than the FMS Bridge visual approach, which provided an
opportunity for an omission error (flight crew inaction). It is also possible that the first officer
missed the information on Air Canada’s FMS Bridge visual approach chart about manually tuning
the ILS frequency because of the presentation and position of that information. Specifically, the
instruction was embedded in the middle of a paragraph on the second (and last) page of the
approach chart, as shown in figure 9, which was not optimal for capturing pilot attention because
the action item could be overlooked. The instruction to manually tune the ILS frequency for the
FMS Bridge visual approach could have been emphasized, for example, as part of a bulleted list,
which Air Canada used in other company procedures to draw pilots’ attention to relevant
information.
The NTSB concludes that the flight crew’s failure to manually tune the ILS frequency for
the approach occurred because (1) the FMS Bridge visual approach was the only approach in
Air Canada’s Airbus A320 database that required manual tuning of a navigation frequency, so the
manual tuning of the ILS frequency was not a usual procedure for the crew, and (2) the instruction
on the approach chart to manually tune the ILS frequency was not conspicuous during the crew’s
review of the chart. Although the incident flight was operating under 14 CFR Part 129, the
approach chart that the flight crew used was originally developed by an air carrier operating under
14 CFR Part 121. Therefore, the NTSB recommends that the FAA work with air carriers
conducting operations under 14 CFR Part 121 to (1) assess all charted visual approaches with a
required backup frequency to determine the FMS autotuning capability within an air carrier’s fleet,
(2) identify those approaches that require an unusual or abnormal manual frequency input, and
(3) either develop an autotune solution or ensure that the manual tune entry has sufficient salience
on approach charts. The NTSB notes that, after the incident, Air Canada revised its procedures so
that the FMS Bridge approach to runway 28R would be flown as an instrument approach. (More
information about Air Canada’s postincident actions can be found in appendix B.)
The NTSB notes that the FAA, as part of its work with the Commercial Aviation Safety
Team (CAST), would be in an ideal position to act on Safety Recommendation A-18-23 through
the CAST safety enhancement process because of the team’s shared interest in mitigating
commercial aviation safety issues.
88
Also, according to the FAA, CAST is moving toward “a
proactive approach that focuses on detecting risk and implementing mitigation strategies before
accidents or serious incidents occur” (FAA 2017).
2.2.3 Initial Approach
Air Canada’s procedures allowed pilots to decide whether to descend using the managed
or open descent autopilot mode. The first officer reported that the approach was conducted using
the open descent mode. With the open descent mode, pitch control maintains the target speed/Mach
number, and autothrust maintains idle thrust. The captain reported that he initially flew the
approach using the selected descent mode, which, according to Air Canada, was synonymous with
the open descent mode. However, the captain also reported that he subsequently flew the approach
using the managed descent mode, which guides an airplane to the deceleration point along the
88
In addition, the FAA has a broader oversight role of ensuring that operational risks are appropriately evaluated
under air carriers’ safety management systems (14 CFR Part 5, “Safety Management Systems”).

NTSB Aircraft Incident Report
43
flightpath that was computed by the FMGS and, unlike the open descent mode, considers speed
and altitude constraints.
The NTSB was unable to determine whether the approach was flown using the open or
managed descent mode because of the differing statements from the captain and the first officer
and the lack of FDR parameters to show flight mode annunciator indications. However, the first
officer perceived that the descent was being flown using the open descent mode, which increased
his workload during a critical phase of flight because he had to ensure, among other things, that
altitude constraints were met. The first officer stated that he thought that it was unusual to use the
open descent mode, but he did not notify the captain about his concern because the procedure was
allowed (until reaching the final waypoint on the approach, F101D). This and other breakdowns
in CRM during the incident flight are discussed in section 2.2.5.
89
The captain flew the FMS Bridge visual approach to runway 28R with the autopilot
engaged until just before F101D. After the airplane reached F101D and the autopilot was
disconnected, the first officer began setting the altitude and heading for a missed approach, which
diverted his attention from monitoring the approach as the captain aligned the airplane with
taxiway C.
90
The NTSB recognizes that the first officer set the missed approach altitude and
heading at an appropriate time (given his perception that the airplane was being flown in the open
descent mode). However, his attention was further diverted from monitoring the approach when
the captain requested that the first officer set the runway heading. The first officer stated that he
had difficulty locating the runway heading information on the approach chart and had to find it on
another chart, which extended the first officer’s heads-down time after the airplane passed F101D.
If the first officer had been monitoring the approach at this point, he might have realized,
among other things, that the ILS frequency and identifier and the runway 28R extended centerline
were not depicted on his PFD.
91
The NTSB concludes that the first officer’s focus on tasks inside
the cockpit after the airplane passed the final waypoint reduced his opportunity to effectively
monitor the approach and recognize that the airplane was not aligned with the intended landing
runway.
2.2.4 Final Approach Segment and Go-Around
The airplane passed F101D at an altitude of about 1,100 ft. Shortly afterward, the captain
noticed lights going across what he perceived to be the runway surface. According to the first
officer, between that time and the time that the airplane descended to an altitude of 600 ft, the
89
Other breakdowns in CRM indicated an apparent lack of preparation for the approach, including both flight
crewmembers’ (1) ineffective review of the runway 28L closure NOTAM before the flight and when ATIS
information Quebec was received and (2) lack of discussion about the runway 28L closure during the approach
briefing.
90
Because the first officer perceived that the approach was being flown using the open descent mode, he would
not have set the missed approach altitude until the airplane reached its minimum altitude for the descent (1,200 ft msl)
or the captain was no longer using the autopilot and flight director for guidance.
91
Air Canada’s stabilized approach criteria for a visual approach included lateral tracking as close as possible to
the extended runway centerline or the published inbound course. However, the flight crew could not have verified that
the airplane was tracking close to the extended runway 28R centerline given that the extended centerline information
would not have been electronically depicted (because the ILS/localizer frequency had not been tuned).

NTSB Aircraft Incident Report
44
captain requested that the first officer contact the tower controller to verify that the runway was
clear. According to the ATC voice recording and the NTSB’s airplane performance study, when
the flight crew transmitted, “we see some lights on the runway there, across the runway. Can you
confirm we’re cleared to land?” the airplane was passing through an altitude of 300 ft.
The controller had scanned the runway just before receiving the flight crew’s transmission.
While receiving the transmission, the controller scanned the ASSC and radar displays to check for
conflicts and scanned runway 28R again. The controller confirmed that the airplane was cleared
to land and stated that no other airplanes were on the runway. At that point, the airplane was
passing through an altitude of 200 ft.
The airplane performance study for this incident showed that ACA759 continued the
approach and flew over the first airplane on taxiway C (UAL1) at an altitude of 100 ft and that the
flight crew initiated a go-around when ACA759 was at an altitude of 89 ft.
92
The airplane
performance study also showed that ACA759 flew over the second airplane on taxiway C
(PAL115) at an altitude of 60 ft before the airplane began climbing, which resulted in only 10 to
20 ft of vertical separation between the ACA759 and PAL115 airplanes. The NTSB concludes that
the flight crew-initiated, low-altitude go-around over the taxiway prevented a collision between
the Air Canada airplane and one or more airplanes on the taxiway. Because of the lack of CVR
data for the incident flight, the NTSB could not determine what information the pilots discussed,
if anything, before and during the go-around. Nevertheless, the NTSB was able to determine the
cues that likely led to the flight crew’s recognition of its alignment error and the crew’s initiation
of the go-around maneuver, as discussed in section 2.3.2.2.
The controller recalled that, when ACA759 was about 1/10 mile on short final, the airplane
looked “extremely strange” regarding its location relative to runway 28R, taxiway C, and the
airplanes along the taxiway. When the UAL1 captain stated, over the tower frequency, “where is
that guy going?” at 2355:59, the controller expressed confusion regarding who had made the
transmission.
93
(The UAL1 captain did not identify himself during the transmission.) At that point,
the controller, who had just checked runway 28R twice, was likely trying to process what he was
seeing and hearing. The controller stated, during a postincident interview, that the transmission
seemed “out of context.”
The controller had no reason to think that ACA759 was lined up with taxiway C before he
observed the airplane looking “extremely strange.” The ACA759 flight crew had reported that the
airplane was on approach to runway 28R, and the ASSC display had previously predicted that the
airplane would be landing on runway 28R. Also, the controller had not previously seen an airplane
align with taxiway C. Further, the distance and angle (parallax) of the tower cab relative to the
approach end of runway 28R and taxiway C would have made it difficult for the controller to
visually recognize that ACA759 was aligned with the taxiway instead of the runway, especially at
night and with the lights from the construction on runway 28L and airport vehicle movements.
92
As previously stated, all altitudes in this report are agl (unless otherwise indicated).
93
The ATC voice recording indicated that, 2 seconds after the UAL1 captain stated, “where is that guy going?”
and 2 seconds before he stated, “he’s on the taxiway,” the controller stated to himself, “who is…talk?”

NTSB Aircraft Incident Report
45
When the UAL1 captain stated, 4 seconds after his first transmission, “he’s on the
taxiway,” the controller might have realized what had happened with ACA759. Because the flight
crew had already begun the go-around maneuver (at 2356:05), the airplane was climbing at the
time of the controller’s go-around instruction (2356:09). The controller subsequently told the
flight crew that the airplane appeared to have been lined up with taxiway C. The NTSB concludes
that the controller responded appropriately once he became aware of the potential conflict. A factor
that precluded the controller from determining sooner that a potential conflict existed was the
ASSC system’s lack of capability to detect a taxiway landing and provide an alert, as discussed
further in section 2.5.2.
2.2.5 Crew Resource Management Breakdown
Air Canada’s CRM manual for pilots and the company’s CRM competency guide
addressed, among other subjects, situational awareness, workload management, active monitoring,
and threat and error management. Several crew actions/inactions during the incident flight
demonstrated breakdowns in CRM, many of which were manifested as noncompliance with
Air Canada’s standard operating procedures. These crew actions/inactions included
• the flight crew’s ineffective review of NOTAMs in the flight release;
• the flight crew’s failure to identify the runway 28L closure information within the ATIS
information;
• the flight crew’s failure to conduct a complete approach briefing;
• the first officer’s failure to manually tune the ILS frequency and the captain’s failure to
verify the tuning of the ILS frequency;
• the first officer’s failure to express concern about the perceived use of the open descent
mode; and
• the captain’s request, at the final waypoint (F101D), for the first officer to set the runway
heading, which took the first officer by surprise and prolonged his heads-down time while
the airplane was aligned with the taxiway.
The captain’s and the first officer’s CRM skills were highly rated by other pilots who had
flown with them. Also, a review of Air Canada’s CRM training program indicated that the
crewmembers received comprehensive CRM training. Thus, although errors indicating
breakdowns in CRM occurred during the incident flight, those errors did not appear to be consistent
with both crewmembers’ performance during other flights (except for a check airman’s report of
the first officer’s performance during a flight) and the CRM training that the crewmembers
received.
94
Possible explanations for the breakdowns in CRM during the incident flight include
94
A check airman who had flown with the first officer when he was attempting to upgrade to captain expressed
concern about the first officer’s situational awareness, as stated in section 1.2.2.
NTSB Aircraft Incident Report
46
fatigue (discussed in section 2.3.3) and the high workload associated with the approach, but the
NTSB could not identify the source of the breakdowns due to the lack of CVR information.
Air Canada’s CRM procedures were designed to reflect a threat and error management
model. According to the top level of the model, flight crews were expected to proactively brief
and mitigate threats before they are encountered. Company procedures required crews to brief
potential threats during the approach briefing. Because both flight crewmembers could not recall
the runway 28L closure NOTAM in the flight release and did not assimilate the runway 28L
closure information included in the ATIS information, they did not identify the runway 28L closure
as a potential threat associated with the approach. (If the flight crew had recalled the runway 28L
closure information and briefed it as a threat, that action should have made the information more
readily accessible for future recall.)
According to the next level of the model, flight crews were expected to respond when an
unexpected threat has occurred and manage the threat so that no error occurs. When the captain
aligned the airplane with taxiway C, he did not have any lateral guidance to indicate that the
airplane was off course because of the first officer’s failure to tune the ILS frequency and the
captain’s failure to verify that the approach was properly set up. Also, the first officer, as the
monitoring pilot, was required to communicate all errors and situational awareness concerns to the
captain. However, the first officer was heads down when the captain aligned the airplane with the
taxiway because of the time that it took the first officer to locate the runway heading information
(in response to the captain’s instruction to set the runway heading) and the time needed for the first
officer to set the missed approach altitude and runway heading. As a result, neither crewmember
realized, once the airplane passed the final waypoint, that the airplane was not aligned with the
intended landing runway.
The threat and error management model further indicated that, if the flight crew
mismanaged the threat, then a procedural, communication, or handling error could occur. If such
an error occurs and the crew traps the error, then safety margins will be maintained. Even though
the tower controller confirmed that runway 28R was clear, the flight crew recognized that
something was not right with the approach about the time that the airplane passed over the seawall.
According to the captain, the first officer called for a go-around at the same time as the captain
initiated the go-around maneuver, thereby preventing a collision on the taxiway.
Even though the flight crew performed a go-around at that point, safety margins were
severely reduced given ACA759’s proximity to the ground (below 100 ft) before the airplane
began climbing and the minimal distance between ACA759 and the airplanes on taxiway C. Thus,
a flight crew-induced aircraft state that compromised safety—the bottom level of the threat and
error management model——resulted from ineffective threat and error management. The NTSB
concludes that errors that the flight crewmembers made, including their false assumption that
runway 28L was open, inadequate preparations for the approach, and delayed recognition that the
airplane was not lined up with runway 28R, reflected breakdowns in CRM and led to minimal
safety margins as the airplane overflew taxiway C.

NTSB Aircraft Incident Report
47
2.3 Reasons for Flight Crew’s Misalignment With Taxiway C
The flight crewmembers had recent experience flying into SFO at night: the captain
reported that he had flown into SFO one or two times during the previous 4 months, and the first
officer was the pilot flying on a flight to SFO 2 nights before the incident. The flight crewmembers’
training records indicated no issues with identifying airport surfaces, flying stabilized approaches,
and flying visual approaches. The incident occurred in night VMC, and no evidence indicated any
obstructions or glare in the cockpit that would have affected the flight crew’s view outside of the
cockpit windows. However, the flight crewmembers were unable to identify the runway 28R
surface (despite the presence of approach and runway lighting) and instead aligned the airplane
with parallel taxiway C. Also, neither crewmember recognized that the airplane was not aligned
with the intended landing runway until the airplane was over the airport surface, at which time the
flight crew initiated a low-altitude go-around. Sections 2.3.1 through 2.3.3 discuss reasons for the
flight crew’s alignment error and the factors that led to the eventual recognition of this error, and
section 2.3.4 discusses the mitigation of such errors.
2.3.1 Flight Crew Awareness of Runway Closure
The flight crew had opportunities before the approach to learn about the runway 28L
closure. The first opportunity occurred before the flight when the crewmembers received the flight
release. Both crewmembers stated that they reviewed NOTAMs in the flight release. However, the
first officer stated that he could not recall reviewing the specific NOTAM that addressed the
runway 28L closure. Also, even though the captain stated that he saw the runway closure
information, his actions in misaligning the airplane demonstrated that he did not recall that
information when it was needed, and he thought that runway 28R was runway 28L. The second
opportunity occurred in flight during the crewmembers’ preparations for the approach to
runway 28R. Both crewmembers recalled reviewing ATIS information Quebec, which they
received via an ACARS message in the cockpit, but neither crewmember recalled reviewing the
specific NOTAM in the ATIS information that described the runway 28L closure.
Because the flight crewmembers either did not review or could not recall the information
about the runway 28L closure, they expected to see two parallel runways while on approach to
SFO and further expected that they would need to fly the approach to the right-side surface.
95
The
flight crew’s recent experience flying into SFO would have reinforced these expectations. For
example, when the first officer flew into SFO 2 nights before the incident, the airplane used for
that flight landed on runway 28R at 2305, which was about 18 minutes before runway 28L was
closed. Also, the captain stated that he had never seen runway 28L “dark” and that none of his
previous landings at SFO occurred when a runway was closed.
A runway closure marker with a flashing white “X” was placed at the threshold of
runway 28L to indicate the runway closure. However, the flashing “X” would not have been in the
flight crew’s direct field of view because the “X” was oriented toward the runway 28L final
95
Industry analysis of traffic patterns at SFO showed that airplanes landing on runway 28R tended to stay more
to the right of course when runway 28L was open than when it was closed.

NTSB Aircraft Incident Report
48
approach corridor and the airplane was not aligned with runway 28L.
96
Also, the flash rate might
have been too slow to capture the crew’s attention.
97
(The conspicuity of the “X” to flight crews
on final approach is further discussed in section 2.6.) The NTSB concludes that the flight
crewmembers’ lack of awareness about the runway 28L closure and the crewmembers’ previous
experience seeing two parallel runways at SFO led to their expectation to identify two runway
surfaces during the approach and resulted in their incorrect identification of taxiway C instead of
runway 28R as the intended landing runway.
The NTSB considered the presentation and priority of the runway 28L closure information
compared with other information that the flight crew received. The flight release package was
27 pages long and consisted of, among other items, route, weather, and NOTAM information. The
NOTAM indicating the runway 28L closure (“RWY 10R/28L CLSD”) appeared on page 8 of the
package, which was also the second page of NOTAM information, under the gray highlighted
heading “DESTINATION” (which appeared on the previous page). Features of the NOTAM text
emphasized the closure information, such as the use of bold font for the words “RWY” and
“CLSD” and a “**NEW**” designation in red font with asterisks before the NOTAM text, as
shown in figure 10.
98
However, this level of emphasis was not effective in prompting the flight
crewmembers to review and/or retain this information, especially given the NOTAM’s location
(toward the middle of the release), which was not optimal for information recall. A phenomenon
known as “serial position effect” describes the tendency to recall the first and last items in a series
better than the middle items (Colman 2006).
The ACARS message providing ATIS information Quebec, as displayed in the cockpit,
was 14 continuous lines with all text capitalized in the same font. As shown in figure 11, the
NOTAM indicating the runway 28L closure appeared at the end of line 8 and the beginning of
line 9. The uniform presentation of the ATIS information could have contributed to the flight
crew’s oversight of the runway closure information. The flight crew’s receipt of ATIS information
Quebec via ACARS was consistent with Air Canada’s procedure to obtain ATIS information using
either ACARS or VHF communications. Thus, effective presentation of information is important
for flight crewmembers who obtain ATIS and other information via ACARS. The capability exists
to make important information more conspicuous in an ACARS message by, for example, inserting
line breaks within the text to group related information.
The NTSB concludes that, although the NOTAM about the runway 28L closure appeared
in the flight release and the ACARS message that were provided to the flight crew, the presentation
of the information did not effectively convey the importance of the runway closure information
and promote flight crew review and retention. Multiple events in the National Aeronautics and
Space Administration’s aviation safety reporting system (ASRS) database showed that this issue
96
The size of the “X,” 20.5 ft by 20.5 ft, would have appeared small along the 200-ft width of runway 28L.
97
The “X” flashed on for 2.5 seconds and off for 2.5 seconds, equating to a frequency of 0.2 Hz. Although a
0.2-Hz flash at the threshold of runway 28L might be effective at preventing the use of the runway when closed, the
frequency might have been too low to have captured the attention of the ACA759 flight crewmembers unless they had
explicitly focused their attention on the approach end of runway 28L.
98
Although the red text would have been visible during the crewmembers’ review of the flight release before
departure, the low ambient lighting conditions in the cockpit would likely have made the red text less conspicuous.

NTSB Aircraft Incident Report
49
has affected other flight crews, indicating that all air carriers could benefit from improved
information display in flight releases and ACARS messages.
99
The way information is presented can significantly affect how information is reviewed and
retained. Specifically, when pilots review information, their scan and retention of that information
is influenced by the pilots’ perceived relevance of the information to a task. Thus, it is possible for
a pilot to miss more relevant information when it is presented with information that is less relevant.
Although human limitations (such as fatigue and time pressure/workload) may affect the review
of information, these limitations can be overcome with effective information presentation. For
example, items in the middle of a list can be better retained if the information is presented with
“intensity” because a sharp, clear, or salient presentation has a better chance of being recalled
compared with less visually stimulating information (FAA 2008). Therefore, the NTSB
recommends that the FAA (1) establish a group of human factors experts to review existing
methods for presenting flight operations information to pilots, including flight releases and general
aviation flight planning services (preflight) and ACARS messages and other in-flight information;
(2) create and publish guidance on best practices to organize, prioritize, and present this
information in a manner that optimizes pilot review and retention of relevant information; and
(3) work with air carriers and service providers to implement solutions that are aligned with the
guidance. The NTSB notes that one way to ensure that air carriers effectively present and prioritize
relevant information in flight releases and ACARS messages would be to develop an industry
standard.
2.3.2 Role of Expectation Bias
2.3.2.1 Initial Taxiway Misalignment
Because the flight crewmembers were not aware of the runway 28L closure, they were
likely expecting SFO to be in its usual configuration, which would include runway 28L being open
for departures and arrivals and airplanes using taxiway F (as shown in figure 3) to reach the
departure end of runway 28L. Because of the runway 28L closure on the night of the incident,
airplanes were using taxiway C to depart from runway 28R.
The flight crewmembers stated, during postincident interviews, that the taxiway C surface
resembled a runway, which they believed was runway 28R. A cue supporting the crewmembers’
perception that they were aligned with runway 28R was the lighting from the airplanes on
taxiway C. Specifically, the airplanes’ wingtip navigation lights would have partially resembled
(width-wise) runway edge lighting.
100
Also, the airplanes’ flashing red beacon lights would have
99
The NTSB conducted an ASRS search to identify reports since 2010 related to flight crew confusion resulting
from the depiction of ACARS messages and/or predeparture flight plan information. The NTSB found multiple reports
of altitude and lateral deviations in which the pilot cited the formatting of information as a related issue, which further
indicates that information display improvements are needed for text-based resources. For more information, see
exemplar cases (ACNs [accession numbers] 1282309, 1409095, 1414185, 1447318, 1540033, 1544364, and 820437)
in the ASRS database (https://asrs.arc.nasa.gov/search/database.html
, accessed September 14, 2018).
100
The second and third airplanes on taxiway C, an Airbus A340 and a Boeing 787, respectively, had wing spans
of about 200 ft, which was also the runway 28R width. (The first airplane on taxiway C, a Boeing 787, also had a wing
span of 200 ft, but the airplane was oriented perpendicularly to the taxiway. Thus, those wingtip lights would not have
created the illusion to the incident flight crewmembers that they had aligned ACA759 with runway 28R.)

NTSB Aircraft Incident Report
50
been consistent with features associated with approach lighting. Another cue that would have
supported the crew’s perception was the presence of runway and approach lights on runway 28R,
which would also have been present on runway 28L when open. However, the runway and
approach lights on runway 28L were off, and the construction lighting that was reported on the
runway 28L surface had features that were consistent with ramp lighting.
A psychological concept associated with perception and decision-making that can allow a
mistaken assessment to persist is expectation bias, which refers to the manipulation of perceived
elements to values consistent with a person’s expectation (Bhattacherjee 2001). A similar concept,
confirmation bias, results from a tendency to primarily seek out confirming evidence of a belief
while spending less effort seeking out negative evidence that can disconfirm the belief (Nickerson
1998). Thus, expectation bias and confirmation bias can cause a person’s incorrect belief to persist
despite available contradictory evidence. Both biases occur as part of basic information processing,
and a person may not be actively aware of such biases at the perceptual level. In this report, the
term “expectation bias” also describes the effects of confirmation bias.
Expectation bias is not a new phenomenon in aviation. The NTSB investigated numerous
accidents and incidents that involved pilot errors resulting from expectation bias, particularly in
night VMC when fewer cues were available to pilots to aid in airport and runway identification.
For example, in January 2014, a Boeing 737 landed at the wrong airport in Branson, Missouri, in
night VMC. The flight crew expected that the visually identified airport and runway were the
intended destination and did not reference cockpit displays to verify the airport and runway. As a
result, the airplane landed on runway 12 at M. Graham Clark Downtown Airport instead of
runway 14 at Branson Airport. Also, in November 2013, a Boeing 747 landed at the wrong airport
in Wichita, Kansas, in night VMC due to the flight crew’s expectation that the observed runway
lights were from the intended landing runway at McConnell Air Force Base. Instead, the airplane
landed at Colonel James Jabara Airport on a runway that was one-half the length of the intended
landing runway. For both of these cases, cues that indicated the flight crew’s mistaken perception
were available; however, those cues were not effectively used because the crewmembers’
expectation bias outweighed the available conflicting cues.
101
For this incident, lighting aids generally associated with runways were not present on
taxiway C. Specifically, although the flight crew perceived the taxiway to be the intended runway,
the taxiway did not have a precision approach path indicator, touchdown zone lights, full-length
edge lights, and approach lights.
102
However, the absence of these normally conspicuous features
of a runway would have been difficult for the flight crewmembers to recognize because of their
expectation bias and the inherent difficulty detecting omissions in the environment (the latter of
which could have been mitigated if the flight crew had briefed the runway 28L closure). In
addition, features present along taxiway C were inconsistent with it being a runway. For example,
although the presence of centerline lights along the full surface length was a cue that was consistent
101
For more information, see NTSB incident numbers DCA14IA037 and DCA14IA016, respectively.
102
Air Canada’s stabilized approach criteria for a visual approach included vertical tracking on approximately a
3° glidepath and using a visual approach slope indicator. Postincident interviews and airplane track data suggested
that the captain used the precision approach path indicator located to the left of runway 28R for glidepath information,
which was intended for airplanes approaching that runway. The availability of this glidepath information while the
airplane was aligned with taxiway C would have supported the flight crew’s expectation that the airplane was aligned
with runway 28R.

NTSB Aircraft Incident Report
51
with a runway, the taxiway centerline lights were green, as shown in figure 4.
103
(Runway
centerline lights are white.) Also, flashing yellow in-pavement guard lights were present on
taxiway C (also shown in figure 4), which would not have been present on a runway surface
because the guard lights were designed to prevent a taxiing airplane from crossing onto a runway.
During postincident interviews, the flight crewmembers recalled seeing specific color
cues, including the green taxiway centerline lights.
104
However, the flight crew continued the
approach despite this conflicting cue. Given that the general outline of airplane lights along
taxiway C (in a straight line) had likely confirmed the crew’s expectation that the right-side surface
was a runway, the omission of conflicting color cues in the crew’s assessment of the runway
environment was consistent with the effects of expectation bias.
105
The captain of DAL521 (the
flight that immediately preceded the ACA759 into SFO) provided a similar assessment during
postincident interviews. Specifically, the DAL521 captain stated that the airplane lights on
taxiway C gave the impression that that surface could have been a runway.
106
Although multiple cues were available to the flight crew to distinguish runway 28R from
taxiway C, sufficient cues also existed to confirm the crew’s expectation that the airplane was
aligned with the intended landing runway. As a result, once the airplane was aligned with what the
flight crewmembers thought was the correct landing surface, they were likely not strongly
considering contradictory information. The NTSB concludes that the cues available to the flight
crewmembers to indicate that the airplane was aligned with a taxiway were not sufficient to
overcome their belief, as a result of expectation bias, that the taxiway was the intended landing
runway.
2.3.2.2 Flight Crew Recognition of Misalignment
The captain stated that, while on final approach, he noticed lights going across what he
thought was the runway 28R surface; this description is consistent with the in-pavement guard
lights on taxiway C. Despite this cue indicating that the airplane was aligned with a taxiway, the
captain’s expectation bias continued because of his assumption that the lights were associated with
an airplane on the runway surface. The captain then asked the first officer to verify with the
controller that the runway was clear. When the first officer looked up after prolonged heads-down
time during the approach (see section 2.2.3), the airplane was lined up with the taxiway. However,
the first officer presumed that the airplane was aligned with runway 28R due, in part, to his
expectation that the captain would align the airplane with the runway, and the first officer did not
103
The NTSB is currently investigating a December 2017 incident involving a Horizon Air Bombardier Q400
that was attempting to land on runway 6 at Pullman-Moscow Regional Airport, Pullman, Washington, at night. The
runway was dark because its lights were out of service, and the airplane landed on the taxiway that was parallel to the
runway despite the illumination of blue taxiway edge lights, which the flight crew perceived as dim white runway
edge lights. For more information, see NTSB incident number DCA18IA081
.
104
Taxiway lighting at YYZ, where the flight crew was based, was similar to the lighting on SFO taxiway C;
both airports had green taxiway centerline lights and blue taxiway edge lights.
105
The airplanes’ wingtip navigation lights were red (left wing) and green (right wing), and the runway edge
lighting was white.
106
The DAL521 captain also stated that, because the lights from the airplanes located on taxiway C were in a
straight line, the airplane lights could have been perceived as centerline lights, which could confuse a flight crew.

NTSB Aircraft Incident Report
52
immediately recognize that the surface ahead was not the intended landing runway. When the first
officer contacted the controller, the airplane was about 4,000 ft (0.66 nm) from the airport seawall.
As ACA759 continued to approach the airport seawall, the flight crew of the second
airplane on taxiway C, PAL115, saw that ACA759 was lined up with taxiway C, and the PAL115
crew turned on that airplane’s landing lights to alert the ACA759 crew. Video information showed
that PAL115’s landing lights illuminated the surface in front of that airplane as well as the tail and
side of the first airplane on taxiway C, UAL1. About this time, the UAL1 captain made the first of
two transmissions, on the tower frequency, about the position of an airplane above the airport
surface; these transmissions were also available cues for the incident flight crew to recognize
ACA759’s misalignment.
107
In addition, about this time, ACA759 descended to an altitude at which its landing lights
would have illuminated the environment below. The appearance of airplanes on the surface
(especially given that the controller had just advised the flight crew that runway 28R was clear)
and the lack of runway markings on the surface should have been additional cues indicating that
the airplane was not aligned with runway 28R.
During postincident interviews, the captain and the first officer were unable to identify a
specific triggering factor in the environment that led to the decision to initiate and call for,
respectively, a go-around. However, all of the cues mentioned above occurred within 6 seconds
before the initiation of the go-around (2355:59 to 2356:05). That period is consistent with the time
for pilots to recognize a cue, make a decision, and execute an action. The NTSB concludes that
multiple salient cues of the surface misalignment were present as the airplane approached the
airport seawall, and one or more of these cues likely triggered the captain’s initiation of a
go-around, which reportedly occurred simultaneously with the first officer’s call for a go-around.
2.3.3 Role of Flight Crew Fatigue
The flight crew’s work schedule for the incident flight complied with the applicable
Canadian flight time limitations and rest requirements (as discussed later in this section). Also, as
previously stated, there was no evidence of sleep disorders or medical conditions that would have
affected the quality of the captain’s and the first officer’s sleep in the days before the incident.
During the 3 days before the incident, the captain had sleep opportunities of between 4.75
and 8 hours. The captain reported that he needed 6 to 7 hours of sleep to feel rested; thus, he did
not likely have a chronic sleep debt, but might have had an acute sleep debt, at the time of the
incident. Information about the first officer’s sleep opportunities was only available for the 2 days
before the incident. During that time, the first officer had sleep opportunities of between 7 and
7.5 hours (including naps). Because the first officer reported that he needed 8 hours of sleep to feel
rested, it is possible that he was experiencing a slight acute or chronic sleep debt at the time of the
107
ACA759 was 500 ft (0.08 nm) from the airport seawall when the UAL1 captain made his first transmission
about the position of an arriving airplane. When the UAL1 captain made his second transmission about the position
of an arriving airplane, ACA759 was 450 ft (0.07 nm) beyond the seawall. The flight crewmembers recalled, during
postincident interviews, that they did not hear specific transmissions on the tower frequency between the controller’s
verification that the runway was clear and his go-around instruction.

NTSB Aircraft Incident Report
53
incident. However, other fatigue factors would have more strongly affected both crewmembers
during the incident flight.
The incident occurred about 2356, which was 0256 EDT according to the flight crew’s
normal body clock time. The captain reported that he typically went to sleep after 0000 EDT, and
the first officer reported that he typically began to feel tired about 2300 EDT. Thus, part of the
incident flight occurred during a time when the flight crew would normally have been asleep. Also,
0256 EDT approximates the start of the human circadian low period described in Air Canada’s
fatigue information (0300 to 0500 body clock time). Even when a person is well rested, operating
during this time of day increases the possibility of performance decrements (Caldwell 1997).
Because the crewmembers were awake at a time that was opposite of their normal body clocks,
they were more vulnerable to the effects of fatigue, which they reported experiencing after
navigating through thunderstorms (about 0045 EDT on July 8) and between 0230 and 0300 EDT
(on July 8).
In addition, at the time of the incident, the captain had been awake for more than 19 hours,
and the first officer had been awake for more than 12 hours. The first officer took advantage of an
opportunity to nap for 1.5 hours before reporting for duty, but the flight crewmembers would likely
not have been able to take advantage of controlled rest during the flight because they were dealing
with thunderstorms during the first half of the flight and preparing for the approach during the
second half of the flight.
108
The NTSB’s January 1994 study of flight crew-related major aircraft
accidents indicated that fatigue related to lengthy periods of wakefulness could contribute to errors.
Specifically, the study found that flight crewmembers who had been awake for more than 11 hours
made significantly more procedural and tactical decision errors than those who had been awake
for less time (NTSB 1994).
Among the performance decrements resulting from fatigue is the inability to adapt behavior
to accommodate new information, which could lead to higher susceptibility for expectation bias
and increased difficulty of overcoming expectation bias once it occurs (Harrison and Horne 1999).
The NTSB concludes that the captain and the first officer were fatigued during the incident flight
due to the number of hours that they had been continuously awake and circadian disruption, which
likely contributed to the crewmembers’ misidentification of the intended landing surface, their
ongoing expectation bias, and their delayed decision to go around.
According to Canadian flight duty time and rest requirements (Canadian Aviation
Regulations 700.16, “Flight Duty Time Limitations and Rest Periods”), the incident flight crew
could have been on duty for 14 hours plus an additional 3-hour extension due to “unforeseen
operational circumstances” (the delayed arrival of the inbound airplane due to weather).
109
Thus,
the incident captain and first officer could have been on duty until 0940 (1240 EDT) on July 8.
The flight crewmembers completed their duty periods at 0032 (0332 EDT) on July 8, which
108
In addition, no evidence indicated that either pilot filed a fatigue report, which Air Canada requests from
flight crewmembers who use the controlled rest policy.
109
According to Canadian Aviation Regulations 700.17, the “maximum flight duty time referred to
in…700.16(1) may be exceeded if…the flight is extended as a result of unforeseen operational circumstances”
Transport Canada’s “Guidance Material Concerning Flight Time and Flight Duty Time Limitations and Rest Periods,”
S740.17, indicated that “unforeseen operational circumstances” relate to circumstances, including weather, that result
in delays to a planned schedule.

NTSB Aircraft Incident Report
54
complied with Canadian regulations, but the regulations would have allowed the crewmembers to
remain on duty for another 9 hours.
The NTSB compared the Canadian flight time and rest requirements with those required
by 14 CFR Part 117, “Flight and Duty Limitations and Rest Requirements: Flightcrew Members.”
This comparison showed that the incident first officer’s flight and duty time and rest requirements
would have complied with the provisions of Part 117.
110
However, the flight and duty time and
rest requirements for the captain, as a company reserve pilot, would not have complied with
Part 117 regardless of whether he would have been considered to have been on long- or short-call
reserve.
111
(Although Part 117 addressed long- and short-call reserve, Canadian regulations did
not make this distinction.) In addition, once assigned a flight, Canadian reserve pilots do not have
any limitations on flight and duty time beyond those for line pilots.
112
For pilots on long-call reserve, 14 CFR 117.21(d) indicated that a flight crewmember must
receive a 12-hour notice of report time if the assigned flight begins before, and operates into, a
flight crewmember’s window of circadian low.
113
The incident captain was assigned to the flight
to SFO at 0849 (1149 EDT) and reported for the flight at 1640 (1940 EDT), resulting in a notice
period of 7 hours 51 minutes. Thus, the notice period would not have complied with US regulations
for long-call reserve. Canadian regulations do not include a limitation on minimum notice of report
time.
For pilots on short-call reserve, 14 CFR 117.21(c)(3) indicated that the total number of
hours that a flight crewmember spends on reserve and on duty cannot exceed 16 hours (from the
beginning of the reserve availability period). The incident captain went on reserve call at 0813
(1113 EDT) on July 7. If the captain had been subject to the flight and duty limitations of Part 117
(and considered to be on short-call reserve), he could operate a flight as long as his duty period
ended before 0013 (0313 EDT) on July 8. Because of the 49-minute takeoff delay, the flight was
projected to arrive at the gate at SFO at 0002 (0302 EDT) with an estimated duty end time of 0017
(0317 EDT), which would have exceeded Part 117 requirements by 4 minutes. To comply with
110
Specifically, 14 CFR 117, Table B, “Flight Duty Period: Unaugmented Operations,” provided the maximum
flight duty period limits (in hours) for line pilots. According to the table, the first officer would have been limited to
12 hours of duty. He worked from 1640 to 0032 (1940 to 0332 EDT), which was a total of 7 hours 52 minutes.
111
According to 14 CFR 117.3, long-call reserve meant that, before beginning the rest period required by
section 117.25, a pilot is notified to report for a flight duty period after the completion of the rest period, whereas
short-call reserve meant a period of time in which a pilot is assigned to a reserve availability period. Generally, pilots
on long-call reserve can be on call for a 24-hour period but, when scheduled, are released from duty and put on rest
for a particular assignment. Pilots on short-call reserve are typically on reserve for a set amount of time each day and
can be required to report to work with short notice.
112
Transport Canada’s “Guidance Material Concerning Flight Time and Flight Duty Time Limitations and Rest
Periods,” S740.21, “Flight Crew Members on Reserve,” indicated the following: “When a flight crew member is on
reserve, an air operator must provide the flight crew member with the opportunity to obtain at least 8 consecutive
hours [of] sleep in any 24 hours by one of the 3 methods indicated in the standard. When that flight crew member is
contacted and required to report for duty during the period of reserve duty, the flight crew member is no longer
considered to be on reserve but on duty…. This means that at anytime during the reserve period, a flight crew member
can be required to start a 14 hour duty period (or longer depending on the applicability of those sections of 700.16 and
720.16 which permit extended flight duty times). A flight crew member therefore must remain rested while on reserve
such that they are able to cope with a full duty day if called.”
113
This section previously described the human circadian low period as between 0300 and 0500 body clock time,
which was consistent with Air Canada’s fatigue guidance and academic research. According to 14 CFR 117.3, the
window of circadian low occurs between 0200 and 0559 body clock time.

NTSB Aircraft Incident Report
55
regulations, the flight would have had to take off by 1854 (2154 EDT); however, the airplane took
off at 1858 (2158 EDT).
114
Transport Canada indicated that its current flight and duty time regulations have been in
effect since 1996. In 2010, the Canadian Aviation Regulatory Advisory Council Working Group
began to update Canada’s regulations relating to fatigue. In 2014, Transport Canada released a
draft of proposed new regulations and, in 2017, revised the draft proposed regulations.
115
According to Transport Canada, the proposed regulations would better address the challenge of
fatigue mitigation for pilots on reserve duty who are called to operate evening flights extending
into their window of circadian low.
The NTSB is aware that the Air Canada Pilots Association and Safer Skies, which
comprises five unions in Canada, have been advocating for stricter rest requirements and flight
time limitations to address pilot fatigue. However, Transport Canada has not yet finalized its
rulemaking in this area. The NTSB concludes that current Canadian regulations do not, in some
circumstances, allow for sufficient rest for reserve pilots, which can result in these pilots flying in
a fatigued state during their window of circadian low. Therefore, the NTSB recommends that
Transport Canada revise current regulations to address the potential for fatigue for pilots on reserve
duty who are called to operate evening flights that would extend into the pilots’ window of
circadian low.
2.3.4 Mitigations to Overcome Expectation Bias
Expectation bias occurs automatically and can be difficult to overcome once established
because of its inherent strength. One way to overcome expectation bias is through training that
stresses active questioning of observations and recognizing the presence of conflicting cues. About
3 months before this incident, Air Canada implemented training on plan continuation and
expectation bias. The training, which was provided to company pilots during annual recurrent
training, comprised a video titled “Understanding Gut Feel,” which explained that a gut feeling
was a sense of knowing things before a person could consciously know, communicate, or explain
them. The video also explained that a gut feeling indicated a potential threat resulting from a
situation that was different or strange or had changed. The NTSB reviewed the video and the
planned PowerPoint presentation (to be introduced during the 2018/2019 training cycle) and found
that they provided a good overview of the hazards of expectation bias and stressed monitoring and
active questioning to mitigate the hazards.
The incident captain and first officer did not receive this training before the incident flight
and were scheduled to receive the training during their next annual recurrent training. Such training
might have provided the captain and first officer with techniques to actively question their
expectations, recognize their error, and act sooner. For example, during postincident interviews,
the first officer stated that, when he looked up after the captain asked him to contact the controller
to verify that the runway was clear, he thought that something was not right but could not resolve
114
If the flight had taken off at 1854 (2154 EDT), the captain would have been in compliance with Part 117
because the delay in his actual duty end time (0032/0332 EDT) occurred due to events after takeoff.
115
Information about the proposed regulations is available at http://www.gazette.gc.ca/rp-pr/p1/2017/2017-07-
01/html/reg2-eng.html (accessed September 14, 2018).
NTSB Aircraft Incident Report
56
what he was seeing. The training video provided pilots with a process for assessing such a feeling.
Specifically, the video presented a basic strategy for listening to gut feelings when evaluating a
situation, as expressed by the acronym “LIVE”: listen (to signals), investigate (what has changed
or is different), validate (test and confirm a theory about what is different), and express
(communicate the concern to others). Although the flight crewmembers eventually recognized
(just before initiating the go-around) that the situation was not what they expected, they missed
opportunities earlier in the approach (as indicated in sections 2.3.1 and 2.3.2) to reassess their
expectations.
In addition to active questioning to overcome expectation bias, which may be prone to
human limitations such as fatigue impairment, cockpit systems to improve crew positional
awareness could provide a conspicuous cue of a misalignment with an intended landing surface.
For example, an EGPWS option developed by Honeywell (known as RAAS) provides
supplemental information to a flight crew about an airplane’s position relative to a runway during
final approach. Studies showed that RAAS was effective in improving pilot performance and
recognition of potential conflicts related to positional awareness (Khatwa 2004).
As a result of its investigation of the August 27, 2006, wrong runway takeoff at Blue Grass
Airport, Lexington, Kentucky, the NTSB recommended (A-07-45) that the FAA “require that all
14 Code of Federal Regulations Part 91K, 121, and 135 operators install on their aircraft cockpit
moving map displays or an automatic system that alerts pilots when a takeoff is attempted on a
taxiway or a runway other than the one intended” (NTSB 2007). In a July 13, 2010, letter regarding
Safety Recommendation A-07-45, the FAA provided details about a program to determine the
effectiveness of cockpit moving map displays and described RAAS as “a product intended to
improve situational awareness by providing pilots with aural advisories.” On April 9, 2014, the
FAA stated that it drafted policy changes based on the lessons learned from the program but that
it had no plans to require the technology requested in the NTSB’s recommendation. As a result,
the NTSB classified Safety Recommendation A-07-45 “Closed—Unacceptable Action” on
July 23, 2014.
Although the FAA has not mandated a system that provides supplemental information to a
flight crew about an airplane’s position relative to a runway during final approach, the
investigation of this incident found a safety benefit of such a system. Specifically, the NTSB asked
Honeywell to conduct a simulation of the incident circumstances with an EGPWS that had the
SmartLanding option, which had some features not provided by RAAS, including an alert for a
potential taxiway landing. The simulation showed that the flight crew would have received the
aural alert “Caution Taxiway, Caution Taxiway” when the airplane was at a radio altitude of 235 ft.
At that point, the airplane would have been 2,600 ft (0.43 nm) from the airport seawall, and the
flight crew would have been required to conduct a go-around because landing could not have been
accomplished within the touchdown zone. Thus, such technology, if it had been installed on the
incident airplane, could have helped the flight crew identify the surface misalignment and could
have resulted in a go-around that was performed at a safer altitude (before the airplane was
dangerously close to other airplanes), thereby improving safety margins.

NTSB Aircraft Incident Report
57
FAA data (as of August 3, 2018) indicated that 85% of wrong surface landings involved
general aviation airplanes.
116
Thus, additional information about an airplane’s position relative to
a runway on final approach would benefit all pilots of airplanes landing at primary airports within
Class B and Class C airspace.
117
The NTSB concludes that flight safety would be enhanced if
airplanes landing at primary airports within Class B and Class C airspace were equipped with a
cockpit system that provided flight crews with positional awareness information that is
independent of, and dissimilar from, the current ILS backup capability for navigating to a runway.
Although Honeywell’s SmartLanding system provides an alert if a potential taxiway
landing is predicted, the NTSB understands (from conversations with the FAA) that there are
current limitations on the widespread implementation of taxiway mapping.
118
However, for a
system that provides an alert when an airplane is not aligned with a runway surface, only the
airplane position and the runway location are required, which are currently available in many
transport-category airplanes. As a result, the NTSB believes that developing a system that provides
an alert for non-runway surface alignment would be feasible in the near term with existing
technology.
119
Therefore, the NTSB recommends that the FAA establish a requirement for
airplanes landing at primary airports within Class B and Class C airspace to be equipped with a
system that alerts pilots when an airplane is not aligned with a runway surface.
The system described in Safety Recommendation A-18-25 would alert if an airplane was
predicted to land on a non-runway surface, such as a taxiway. The NTSB recognizes that the
technology for a system that provides an alert to pilots when an airplane is not aligned with the
intended runway surface may not currently be available. Such a system would also need to define
and compare information about the intended runway (from ATC clearance instructions and/or the
airplane’s navigation system) with the airplane’s runway alignment on final approach.
116
The FAA’s data also showed that 85% of wrong surface landings involved ATCT facilities that were
considered to be between levels 4 and 9, indicating operations at small- or medium-sized ATCT facilities. These
facilities might not have as many controllers and some of the equipment that level 10 through 12 ATCT facilities have.
Thus, it is important for pilots operating at airports with level 4 through 9 ATCT facilities to have cockpit technology
to aid in determining an airplane’s position relative to a runway on final approach.
117
According to the FAA, primary airports have more than 10,000 passenger boardings (enplanements) each
year. Per the FAA’s Aeronautical Information Publication, Class B airspace is generally “surrounding the nation’s
busiest airports in terms of IFR operations or passenger enplanements.” Class C airspace is generally “surrounding
those airports that have an operational control tower, are serviced by a radar approach control, and that have a certain
[minimum] number of IFR operations or passenger enplanements.”
118
The FAA indicated that one limitation is getting teams from (or contracted by) the FAA to every airport in
the FAA’s database to survey taxiways, which would be a significant undertaking for a benefit that could be gained
by installing a cockpit system that provides flight crews with positional awareness information by notifying them
when an airplane is not aligned with a runway surface.
119
The NTSB is investigating the August 10, 2018, incident involving a Gulfstream IV airplane operated by
Pegasus Elite Aviation as PEGJET flight 19 at Philadelphia International Airport, Philadelphia, Pennsylvania. The
airplane, which was operating under 14 CFR Part 135 as a charter flight, was cleared to land on runway 35 about
2050 EDT. During the visual approach, the airplane aligned with taxiway E. About 0.1 mile from the end of taxiway E,
the pilot initiated a go-around, and the airplane overflew four air carrier airplanes on taxiway E during the climb. The
incident airplane came within about 200 ft of the first airplane on the taxiway. At the time of the approach, the runway
35 runway end identifier lights and the precision approach path indicator lights were out of service. The seven airplane
occupants were not injured, and the airplane was not damaged. For more information, see NTSB incident number
DCA18IA265
. The circumstances of this incident demonstrate the importance of equipping airplanes with additional
positional awareness technology when landing at primary airports in Class B and Class C airspace because of the risk
to passengers in airplanes on a taxiway.

NTSB Aircraft Incident Report
58
Honeywell’s systems are examples of existing technology that can accurately identify a
runway surface when a pilot is on final approach.
120
However, the NTSB is not aware of an
automated system that has reliably demonstrated the ability to indicate whether an airplane is
aligned with the specific runway for which it has been cleared. Such a system would further
improve safety, especially at airports with parallel runways (which, according to the FAA’s wrong
surface landing video, account for 75% of wrong surface landings), and provide a longer term and
more robust solution to wrong surface landings. Therefore, the NTSB recommends that the FAA
(1) collaborate with aircraft and avionics manufacturers and software developers to develop the
technology for a cockpit system that provides an alert to pilots when an airplane is not aligned with
the intended runway surface and (2) once such technology is available, establish a requirement for
the technology to be installed on airplanes landing at primary airports within Class B and Class C
airspace.
2.4 Reporting of the Incident Flight
Air Canada’s Flight Operations Manual stated that pilots were to report any accident,
incident, emergency, or other safety-related event (which might require investigating, monitoring,
or tracking) to company flight dispatch as soon as possible. Examples of reportable events included
a significant navigation error, an unstable approach, a go-around, and any hazard that poses a direct
threat to flight safety. Because all of these events occurred during the incident flight, the flight
crew was required to report the incident, but Air Canada’s procedures at the time of the incident
did not indicate what “as soon as possible” meant regarding the specific timeframe for reporting
events.
The captain stated that he did not report the incident to company dispatch shortly after it
occurred because he was “very tired” and it was “very late.”
121
No available evidence indicated
that the flight crew was aware at that point that ACA759 had overflown four air carrier airplanes
positioned along taxiway C; specifically, the crewmembers reported (during postincident
interviews) that they did not see any airplanes on the taxiway, and the controller’s transmission to
the crew about the misalignment did not mention any airplanes positioned on the taxiway. At 0747
on the morning after the incident (July 8), the incident airplane (flown by another flight crew)
departed SFO for Montreal, Canada. The incident captain and first officer met at 1100 on the
morning after the incident to discuss the facts surrounding the event for the ASR. Air Canada
records showed that the captain reported the event to dispatch at 1608. (At that time, the captain
and the first officer would have been preparing for the flight from SFO to YYZ, which departed at
1649.)
According to the dispatcher who received the initial notification about the event, the
captain reported that the airplane was lined up with the wrong runway and that a go-around was
performed. The dispatcher also stated that the captain’s report sounded “innocuous” given the
amount of time (16 hours) that had elapsed since the event. However, Air Canada senior personnel
first learned about the severity of the event—the proximity of the incident airplane to the airplanes
120
As stated in section 1.5.2, Garmin also has such a system available, and Rockwell Collins has a system in
development.
121
The flight crew could have sent an ACARS message to report the event in a timely manner.

NTSB Aircraft Incident Report
59
on the taxiway—when the TSB sent an e-mail about 2200 EDT on July 9 that advised company
personnel about the incident circumstances.
122
The Air Canada A320 assistant chief pilot stated
that, during a meeting on July 10, the flight crewmembers were told that ACA759 had overflown
airplanes on a taxiway and that the crewmembers’ responses were “shock” and “surprise.” (The
NTSB could not determine if the flight crew was aware, before this meeting, that ACA759 had
flown over airplanes on taxiway C.)
Air Canada’s director of corporate safety, investigation, and research stated that the
incident airplane had flown about 40 hours before Air Canada senior officials became aware of the
severity of the incident and realized that data from the airplane needed to be retrieved. However,
by that point, the CVR information from the incident flight had been overwritten; the CVR
installed in the incident airplane was designed to record 2 hours of operational data.
123
CVR data for this incident would have provided additional information about the
circumstances leading to the overflight, including the flight crew’s verbalized approach
preparations (during approach set up and approach review) and the timing of pertinent
conversations, such as when the captain asked the first officer to verify that the runway was clear
and when the first officer called for the go-around (compared with when the captain initiated the
go-around). In addition, CVR information would have allowed the NTSB to (1) determine the
timing and content of the flight crew’s conversations during final approach and for any
conversations during and after the go-around and (2) assess the flight crew’s CRM, workload, and
fatigue according to verbalized information and cockpit sounds. The NTSB concludes that,
although the investigation into this incident identified significant safety issues, CVR information,
had it been available, could have provided direct evidence regarding the flight crew’s approach
preparation, cockpit coordination, perception of the airport environment, and decision-making.
2.5 Air Traffic Control Services
2.5.1 Air Traffic Control Tower Midnight Shift Staffing
On the night of the incident, the SFO ATCT was staffed with two controllers for the
midnight shift, which began at 2230 and ended at 0630 the next day. Before the incident occurred,
the controllers evaluated the traffic complexity and determined that the traffic volume would allow
ATCT staffing to be reduced to a single-person operation (which was authorized for midnight shift
staffing), with one controller working all positions in the tower cab and the other controller taking
a recuperative break in the ATCT building. All control positions and frequencies were combined
and operated from the local control position starting about 2349, which was 7 minutes before the
incident occurred.
The controller provided no indications, during a postincident interview, that the
single-person operation affected his workload at the time of the incident. The controller stated that
122
As previously stated, the NTSB learned about this incident from the FAA at 1630 EDT on July 9 and notified
the TSB at 1840 EDT the same day.
123
In 2016, the International Civil Aviation Organization adopted a new standard calling for the installation of
CVRs capable of recording the last 25 hours of aircraft operation on all aircraft manufactured after January 1, 2021,
with a maximum certificated takeoff mass over 27,000 kg engaged in commercial transport.
NTSB Aircraft Incident Report
60
he would not combine positions unless he was comfortable and had some predictability about the
tasks that he would need to perform. He also stated that the traffic volume on the night of the
incident was normal and that he was not overly busy, even with the various frequencies that he
was monitoring. The controller further stated that, if the traffic had become too busy or complex,
he would have asked the other on-duty controller to return to the tower cab to assist. (The other
on-duty controller returned to the tower cab at the end of his recuperative break at 0300 on July 8.)
In addition, analysis of the ATC voice recording indicated that the controller was calm and engaged
during transmissions while ACA759 was on approach through the time that the UAL1 captain
asked where the arriving airplane was going. Thus, the controller’s confusion that resulted from
that transmission was most likely due to the situation and not his workload.
During postincident interviews, pilots of airplanes positioned along taxiway C suggested
that ATCT staffing at the time of the incident was not adequate. Specifically, the UAL1118 captain
stated that the tower controller “was performing way too many functions,” and a UAL863 pilot
stated that the tower controller “should not have been the only controller working the entire
airport.” Although no evidence indicated that ATC workload was a factor in this incident, the
decision to combine local and non-local positions led to congestion on the tower frequency.
Specifically, postincident interviews with the ACA759 flight crew indicated that the first officer
waited to contact the controller (to confirm that the runway was clear) because the tower frequency
was busy. The ATC voice recording showed that, during the 61 seconds before the flight crew’s
query to the controller (from 2354:44 to 2355:45), there were ongoing communications between
the tower and airplanes on the ground.
Given the congestion on the tower frequency, it is possible that the ACA759 flight crew
was waiting for a pause in the conversations between the controller and pilots of airplanes on the
ground but then decided to break into a conversation to relay the crew’s concern about the
perceived lights on the runway. The ATC recording showed that, when the ACA759 flight crew
began its transmission to query whether runway 28R was clear, another pilot was talking to the
controller. However, the controller clearly heard the transmission from ACA759 given that he
checked the status of runway 28R and responded to ACA759’s query 1 second after the flight crew
completed its transmission.
According to postincident interviews, the captain’s request for the first officer to verify
with the controller that runway 28R was clear occurred between the time that the airplane passed
F101D (at an altitude of about 1,100 ft) and the time that the airplane reached an altitude of 600 ft.
The airplane descended below 600 ft at 2355:07, so the flight crew did not break into the
conversation until 38 seconds later. The airplane performance study for this incident found that,
when the flight crew acknowledged the controller’s transmission that the runway was clear, the
airplane was about 500 ft (0.08 nm) from the airport seawall. If the local (tower) and ground control
positions had not been combined, the flight crewmembers would likely have had the opportunity
to communicate their concern earlier. The NTSB concludes that, once the flight crewmembers
perceived lights on the runway, they decided to contact the controller to ask about the lights;
however, their query was delayed because of congestion on the tower frequency, which reduced
the time available for the crewmembers to reconcile their confusion about the lights with the
controller’s confirmation that the runway was clear.
NTSB Aircraft Incident Report
61
At the time of the incident, the SFO ATCT’s standard operating procedures described
staffing requirements between 0630 and 2200 but did not provide such requirements between 2200
and 0630 the next day. After the incident, the SFO ATCT acting air traffic manager issued
guidance that stated that the local and ground control positions could not be combined before 0015.
In response to the NTSB’s June 2018 query about the significance of the 0015 time (which is
26 minutes after the reported time that all positions were combined on the night of the incident),
the SFO ATCT operations manager indicated that 0015 was determined to be the earliest time that
the positions could be combined based on normal traffic patterns, runway closures, administrative
duties, and fatigue guidance.
The SFO ATCT’s standard operating procedures also did not describe the procedures to be
used (and not to be used) during the midnight shift, including those for single-person operations
with combined positions. While working single-person operations on the night of the incident, the
controller applied LUAW procedures. However, FAA Order JO 7210.3Z stated that, when
conducting LUAW operations, the local control position should not be combined with any
non-local control position. Thus, LUAW procedures should not have been used at that point.
The controller was aware that LUAW operations should not be conducted when the local
and ground control positions were combined. However, during a postincident interview, the
controller stated, “when aircraft were on a 5-mile final and compressing, it was hard to fit in a
departure from runway 1, without using LUAW.” The SFO acting air traffic manager stated that,
if LUAW procedures were needed to efficiently move traffic, then traffic was “too busy to combine
positions” into a single-person operation. Thus, the NTSB concludes that, although the use of
LUAW procedures during single-person ATC operations was not a factor in this incident, the tower
controllers should have delayed consolidating local and non-local control positions until LUAW
procedures were no longer needed. The SFO acting air traffic manager stated that, after the
incident, ATCT management had been reemphasizing the correct application of LUAW
procedures.
2.5.2 Airport Surface Surveillance Capability System
The ASSC system was designed to detect aircraft, vehicles, and other objects on the surface
of an airport and present those images on a tower display. If the ASSC system detected a situation
involving two tracks on a runway (aircraft/aircraft, aircraft/vehicle, or aircraft/other tangible
object) and predicted an imminent collision, the system would produce a visual and an aural alarm.
However, the ASSC system was not designed to predict an imminent collision involving an
arriving airplane lined up with a taxiway, so the system functioned as designed and did not produce
an alarm as ACA759 approached taxiway C. The system also functioned as designed during the
12-second period when the ACA759 data block was not shown on the ASSC display (while the
airplane was on short final) because the airplane was not in the system’s depiction area (coverage
cone) during that time.
The controller stated that he noticed that the ACA759 data block had disappeared from the
ASSC display, but he was not concerned about that because he could see the airplane out of the

NTSB Aircraft Incident Report
62
tower cab windows.
124
The ACA759 data block reappeared on the ASSC display just before the
flight crew initiated a go-around. Although the disappearance of the ACA759 data block from the
ASSC display did not contribute to the incident, the current design of the ASSC system does not
assist a tower controller in detecting potential taxiway landings. Such capability would be
especially critical during nighttime and poor visibility conditions when a controller might not be
able to visually observe an airplane lining up with a taxiway.
The ASSC system was one of three ASDE systems in the national airspace system; the
other two were ASDE-3 and ASDE-X. As a result of an October 2009 taxiway landing involving
a Boeing 767 at Hartsfield Jackson Atlanta International Airport, Atlanta, Georgia, the NTSB
recommended in March 2011 that the FAA expand ASDE-X capabilities to detect taxiway
landings by taking the following actions:
125
Perform a technical review of Airport Surface Detection Equipment—Model X to
determine if the capability exists systemwide to detect improper operations such as
landings on taxiways. (A-11-12)
At those installation sites where the technical review recommended in Safety
Recommendation A-11-12 determines it is feasible, implement modifications to
Airport Surface Detection Equipment—Model X to detect improper operations,
such as landings on taxiways, and provide alerts to air traffic controllers that these
potential collision risks exist. (A-11-13)
On May 13, 2011, the FAA stated that “the ability to accurately predict that an aircraft is
arriving to a taxiway is not possible without significant degradation in performance, timeliness,
and accuracy of safety logic alerts for the more likely event of an aircraft arriving to a closed or
occupied runway.” The FAA also stated that those performance tradeoffs existed at some airports
with close parallel and offset threshold runways. The FAA further stated that implementing the
recommended actions could (1) degrade the ASDE-X’s ability to provide correct and timely
predictions to the associated parallel runway, (2) result in additional false alerts due to incorrectly
predicting an aircraft landing on a taxiway, and (3) cause an actual alert to be missed if a runway
is occupied at the time of an incorrect taxiway landing prediction. The FAA planned no further
action regarding the recommendations.
On September 14, 2011, the NTSB noted the FAA’s intent not to implement the
recommended actions and recognized that the recommended review would need to consider
performance tradeoffs, including those that the FAA discussed in its letter. However, the NTSB
stated that the FAA determined, without performing the recommended review, that the
performance tradeoffs would outweigh the safety benefits of providing the recommended
124
The primary responsibility of the local controller was to observe traffic outside of the tower cab window. The
local controller could use the ASSC display and the radar display in the ATCT to augment visual observations of
departing and arriving aircraft as well as aircraft and vehicle movements on runways, taxiways, and other parts of the
movement area.
125
(a) For more information about this incident, see NTSB incident number OPS10IA001. (b) When these
recommendations were issued, the ASSC system had not yet been developed.
NTSB Aircraft Incident Report
63
capabilities, which was not an acceptable response to the recommendations. Accordingly, the
NTSB classified Safety Recommendations A-11-12 and -13 “Closed—Unacceptable Action.”
Since that time, technology has advanced considerably. The FAA’s February 2018 tests at
SEA provided promising results regarding the potential of the ASDE-X system to detect and
predict taxiway landings with only a negligible number of nuisance or false alarms. As previously
stated, the ASDE-X system at SEA was configured to apply the same parameters that are used to
predict a landing on a closed runway, and the tests showed that the system predicted the potential
taxiway landings and provided an ASDE-X alarm when the airplane was within 20 seconds or
3,000 ft of landing. The tests also showed that the alarm occurred with enough time for ATC
personnel to respond, and no false alarms occurred during any of the approaches and taxiway
landing scenarios. Thus, the results of the tests at SEA demonstrated that the concerns that the FAA
expressed in its response to Safety Recommendations A-11-12 and -13 appear to have been
resolved. According to the FAA, a software enhancement, the taxiway arrival prediction capability,
was implemented at SEA in May 2018, and the FAA has a schedule to evaluate the remaining
ASDE-X-equipped airports and implement the software enhancement, where feasible, by the end
of fiscal year 2020.
The NTSB concludes that, if an airplane were to align with a taxiway, an automated ASDE
alert would assist controllers in identifying and preventing a potential taxiway landing as well as
a potential collision with aircraft, vehicles, or objects that are positioned along taxiways. The
taxiway arrival prediction capability that was implemented at SEA (and was scheduled to be
evaluated and implemented at other feasible ASDE-X locations) could be expanded to other ASDE
system models (ASDE-3 and ASSC). Therefore, the NTSB recommends that the FAA modify
ASDE systems (ASDE-3, ASDE-X, and ASSC) at those locations where the system could detect
potential taxiway landings and provide alerts to air traffic controllers about potential collision
risks.
2.6 Runway Closure Markers
A runway closure marker with a lighted flashing white “X” appeared at the approach and
departure ends of runway 28L when it was closed, including on the night of the incident. The
lighted “X” was consistent with the specifications in FAA AC 150/5345-55A, “Specification for
L-893, Lighted Visual Aid to Indicate Temporary Runway Closure.” Although the runway closure
marker might have been effective at preventing a takeoff from or a landing on runway 28L when
it was closed (the specific risks that the lighted “X” was designed to address), the runway closure
marker did not capture the attention of the incident flight crew as the airplane approached the
airport while aligned with taxiway C.
The lighted “X” runway closure marker was not designed to address the possibility that a
flight crew could misidentify a runway surface due to ineffective signaling of a runway closure.
Although air traffic controllers can provide instructions to pilots about the closure of a runway,
NOTAMs and ATIS broadcasts/messages are the primary means to inform pilots about runway
closures. However, the information about runway closures provided in NOTAMs and ATIS
broadcasts/messages is not necessarily a reliable means for ensuring that pilots are aware of the
NTSB Aircraft Incident Report
64
closure information.
126
As previously stated, although the runway 28L closure on the night of the
incident was indicated in NOTAM and ATIS information that the incident flight crew received,
that information was not effective in preventing the flight crew from misaligning the airplane
during the approach to runway 28R.
127
The incident flight crew and the flight crew of DAL521 (which landed on runway 28R
about 4 minutes before the incident occurred) stated that they did not see a lighted “X” on
runway 28L to indicate that it was closed. Given the current specifications for the runway closure
marker, these flight crews likely did not see the “X” because their airplanes were not aligned with
runway 28L. This situation highlights the need for a surface-based system with conspicuous and
unambiguous visual cues that clearly indicate when a runway is closed, even if an approaching
airplane is not aligned with the closed runway. Such a system would provide redundancy in case
a flight crew does not review or retain runway closure information presented in NOTAMs or ATIS
broadcasts/messages. Such a system would also be especially critical in situations involving the
closure of a runway at an airport with parallel landing and taxiway surfaces (such as SFO).
As previously discussed, cockpit mitigations (such as the use of navigational aids to back
up a visual approach to the intended landing runway, as used by the DAL521 flight crew, and a
system to provide additional positional awareness information) and ATC systems to alert
controllers about a potential runway misalignment or taxiway alignment can provide multiple
layers of protection to prevent a flight crew surface alignment error. In addition, when closed
runways are marked conspicuously, the view outside the cockpit (during VMC) of an airport
environment can assure flight crews that an airplane is correctly aligned with a parallel landing
runway.
If the incident flight crewmembers had observed the runway 28L closure marker early in
the approach, their mistaken perception of the airport environment and alignment with taxiway C
might not have occurred. Further, if the runway 28L closure marker had captured the incident
flight crew’s attention later in the approach, that information might have been sufficient for the
crewmembers to detect their mistaken perception and respond to the situation before the airplane
reached the seawall.
The NTSB is not aware of any operational or human factors research to improve the
conspicuity of L-893 runway closure markers during the 31 years since the FAA issued a technical
report about its research on runway closure markers (other than subsequent research on the use of
light-emitting diode bulbs). During that time, widespread advances in lighting and control
126
The NTSB investigated a September 25, 2001, incident in which a Boeing 757 took off from a closed runway
at Denver International Airport, Denver, Colorado. A system failure affected the availability of a NOTAM about the
runway closure, and a controller cleared the airplane to take off from the closed runway. After that incident, the flight
crewmembers stated that they were unaware that the runway was closed, and the captain did not recall if the runway
closure information was included in the ATIS broadcast. As a result of the incident, the NTSB recommended that the
FAA “require the use of physical devices or other means to clearly indicate to flight crews of arriving and departing
aircraft that a runway is closed” (A-03-5
). In response, the FAA issued AC 150/5370-2F, “Operational Safety on
Airports During Construction,” which indicated that airports should use physical devices or other means to indicate
to flight crews that a runway is closed. The NTSB classified Safety Recommendation A-03-5 “Closed—Acceptable
Action” on January 30, 2012.
127
The NTSB has investigated other events in which pertinent NOTAM information was missed; for example,
see NTSB accident numbers DFW07CA092, CEN12LA229, and CEN14FA505.
NTSB Aircraft Incident Report
65
technology have occurred. These advances could allow more conspicuous attentional capture
features to be incorporated into a runway closure marker’s design. Such features, which include
varying the flash pattern, incorporating strobe lights, and/or creating apparent movement, might
direct a pilot’s attention to a closed runway better than the current design of the lighted “X.”
The NTSB concludes that increased conspicuity of runway closure markers, especially
those used in parallel runway configurations, could help prevent runway misidentification by flight
crews while on approach to an airport. Therefore, the NTSB recommends that the FAA (1) conduct
human factors research to determine how to make a closed runway more conspicuous to pilots
when at least one parallel runway remains in use and (2) implement a method to more effectively
signal a runway closure to pilots during ground and flight operations at night.
NTSB Aircraft Incident Report
66
3. Conclusions
3.1 Findings
1. None of the following were factors in this incident: (1) flight crew qualifications, which
were in accordance with Canadian and US regulations; (2) flight crew medical conditions;
(3) airplane mechanical conditions; and (4) airport lighting, which met US regulations.
2. The first officer did not comply with Air Canada’s procedures to tune the instrument
landing system (ILS) frequency for the visual approach, and the captain did not comply
with company procedures to verify the ILS frequency and identifier for the approach, so
the crewmembers could not take advantage of the ILS’s lateral guidance capability to help
ensure proper surface alignment.
3. The flight crew’s failure to manually tune the instrument landing system (ILS) frequency
for the approach occurred because (1) the Flight Management System Bridge visual
approach was the only approach in Air Canada’s Airbus A320 database that required
manual tuning of a navigation frequency, so the manual tuning of the ILS frequency was
not a usual procedure for the crew, and (2) the instruction on the approach chart to manually
tune the ILS frequency was not conspicuous during the crew’s review of the chart.
4. The first officer’s focus on tasks inside the cockpit after the airplane passed the final
waypoint reduced his opportunity to effectively monitor the approach and recognize that
the airplane was not aligned with the intended landing runway.
5. The flight crew-initiated, low-altitude go-around over the taxiway prevented a collision
between the Air Canada airplane and one or more airplanes on the taxiway.
6. The controller responded appropriately once he became aware of the potential conflict.
7. Errors that the flight crewmembers made, including their false assumption that runway 28L
was open, inadequate preparations for the approach, and delayed recognition that the
airplane was not lined up with runway 28R, reflected breakdowns in crew resource
management and led to minimal safety margins as the airplane overflew taxiway C.
8. The flight crewmembers’ lack of awareness about the runway 28L closure and the
crewmembers’ previous experience seeing two parallel runways at San Francisco
International Airport led to their expectation to identify two runway surfaces during the
approach and resulted in their incorrect identification of taxiway C instead of runway 28R
as the intended landing runway.
NTSB Aircraft Incident Report
67
9. Although the notice to airmen about the runway 28L closure appeared in the flight release
and the aircraft communication addressing and reporting system message that were
provided to the flight crew, the presentation of the information did not effectively convey
the importance of the runway closure information and promote flight crew review and
retention.
10. The cues available to the flight crewmembers to indicate that the airplane was aligned with
a taxiway were not sufficient to overcome their belief, as a result of expectation bias, that
the taxiway was the intended landing runway.
11. Multiple salient cues of the surface misalignment were present as the airplane approached
the airport seawall, and one or more of these cues likely triggered the captain’s initiation
of a go-around, which reportedly occurred simultaneously with the first officer’s call for a
go-around.
12. The captain and the first officer were fatigued during the incident flight due to the number
of hours that they had been continuously awake and circadian disruption, which likely
contributed to the crewmembers’ misidentification of the intended landing surface, their
ongoing expectation bias, and their delayed decision to go around.
13. Current Canadian regulations do not, in some circumstances, allow for sufficient rest for
reserve pilots, which can result in these pilots flying in a fatigued state during their window
of circadian low.
14. Flight safety would be enhanced if airplanes landing at primary airports within Class B and
Class C airspace were equipped with a cockpit system that provided flight crews with
positional awareness information that is independent of, and dissimilar from, the current
instrument landing system backup capability for navigating to a runway.
15. Although the investigation into this incident identified significant safety issues, cockpit
voice recorder information, had it been available, could have provided direct evidence
regarding the flight crew’s approach preparation, cockpit coordination, perception of the
airport environment, and decision-making.
16. Once the flight crewmembers perceived lights on the runway, they decided to contact the
controller to ask about the lights; however, their query was delayed because of congestion
on the tower frequency, which reduced the time available for the crewmembers to reconcile
their confusion about the lights with the controller’s confirmation that the runway was
clear.
17. Although the use of line up and wait (LUAW) procedures during single-person air traffic
control operations was not a factor in this incident, the tower controllers should have
delayed consolidating local and non-local control positions until LUAW procedures were
no longer needed.
NTSB Aircraft Incident Report
68
18. If an airplane were to align with a taxiway, an automated airport surface detection
equipment alert would assist controllers in identifying and preventing a potential taxiway
landing as well as a potential collision with aircraft, vehicles, or objects that are positioned
along taxiways.
19. Increased conspicuity of runway closure markers, especially those used in parallel runway
configurations, could help prevent runway misidentification by flight crews while on
approach to an airport.
3.2 Probable Cause
The National Transportation Safety Board determines that the probable cause of this
incident was the flight crew’s misidentification of taxiway C as the intended landing runway,
which resulted from the crewmembers’ lack of awareness of the parallel runway closure due to
their ineffective review of notice to airmen (NOTAM) information before the flight and during the
approach briefing. Contributing to the incident were (1) the flight crew’s failure to tune the
instrument landing system frequency for backup lateral guidance, expectation bias, fatigue due to
circadian disruption and length of continued wakefulness, and breakdowns in crew resource
management and (2) Air Canada’s ineffective presentation of approach procedure and NOTAM
information.
NTSB Aircraft Incident Report
69
4. Recommendations
As a result of this investigation, the National Transportation Safety Board recommends the
following:
To the Federal Aviation Administration:
Work with air carriers conducting operations under Title 14 Code of Federal
Regulations Part 121 to (1) assess all charted visual approaches with a required
backup frequency to determine the flight management system autotuning capability
within an air carrier’s fleet, (2) identify those approaches that require an unusual or
abnormal manual frequency input, and (3) either develop an autotune solution or
ensure that the manual tune entry has sufficient salience on approach charts.
(A-18-23)
Establish a group of human factors experts to review existing methods for
presenting flight operations information to pilots, including flight releases and
general aviation flight planning services (preflight) and aircraft communication
addressing and reporting system messages and other in-flight information; create
and publish guidance on best practices to organize, prioritize, and present this
information in a manner that optimizes pilot review and retention of relevant
information; and work with air carriers and service providers to implement
solutions that are aligned with the guidance. (A-18-24)
Establish a requirement for airplanes landing at primary airports within Class B and
Class C airspace to be equipped with a system that alerts pilots when an airplane is
not aligned with a runway surface. (A-18-25)
Collaborate with aircraft and avionics manufacturers and software developers to
develop the technology for a cockpit system that provides an alert to pilots when
an airplane is not aligned with the intended runway surface, and, once such
technology is available, establish a requirement for the technology to be installed
on airplanes landing at primary airports within Class B and Class C airspace.
(A-18-26)
Modify airport surface detection equipment (ASDE) systems (ASDE-3, ASDE-X,
and airport surface surveillance capability) at those locations where the system
could detect potential taxiway landings and provide alerts to air traffic controllers
about potential collision risks. (A-18-27)
NTSB Aircraft Incident Report
70
Conduct human factors research to determine how to make a closed runway more
conspicuous to pilots when at least one parallel runway remains in use, and
implement a method to more effectively signal a runway closure to pilots during
ground and flight operations at night. (A-18-28)
To Transport Canada:
Revise current regulations to address the potential for fatigue for pilots on reserve
duty who are called to operate evening flights that would extend into the pilots’
window of circadian low. (A-18-29)
BY THE NATIONAL TRANSPORTATION SAFETY BOARD
ROBERT L. SUMWALT, III
Chairman
EARL F. WEENER
Member
BRUCE LANDSBERG
Vice Chairman
T. BELLA DINH-ZARR
Member
JENNIFER HOMENDY
Member
Adopted: September 25, 2018

NTSB Aircraft Incident Report
71
Board Member Statements
Vice Chairman Landsberg filed the following concurring statement on October 4, 2018:
Vice Chairman Bruce Landsberg
Concurring Statement – Air Canada Taxiway Overflight Investigation
Concurring statements for SFO
This incident report should be required reading for all pilots. Only a few feet of separation
prevented this from possibly becoming the worst aviation accident in history. I have some
reservations about some of our recommendations where we may have gone farther than necessary
in some cases and not far enough in others. Time will tell if we got it right.
Recommendation A-18-24 to the FAA on Preflight Information:
From a human factors perspective, the preflight briefing system is archaic and poorly designed.
This Air Canada crew missed two warnings about the closed runway in SFO, first in pre-departure
and secondly, via ACARS before landing. Concerns about legal liability rather than operational
necessity, drive the current system to list every possible Notice to Airmen (Notam) that could,
even under the most unlikely circumstance, affect a flight.
The current system prioritizes protecting the regulatory authorities and airports. It lays an
impossibly heavy burden on individual pilots, crews and dispatchers to sort through literally
dozens of irrelevant items to find the critical or merely important ones. When one is invariably
missed, and a violation or incident occurs, the pilot is blamed for not finding the needle in the
haystack!
GPS and TFR notices often fall into the same category of overly complex and geographically
irrelevant. The legalistic descriptions of TFRs and poorly-descriptive GPS outage areas are
worthless to pilots and dispatchers without tremendous and time-consuming effort. A graphic
presentation of where a flight might be restricted or impacted should be easily found on FAA’s
website and suffice as an official brief. It should also be disseminated to other preflight or
electronic Flight bag providers and be both accurate and timely. FAA should not be allowed to
hide behind FSS using this disclaimer which currently appears on the official FAA TFR website.
“Depicted TFR data may not be a complete listing. Pilots should not use the information on this website for flight planning
purposes. For the latest information, call your local Flight Service Station at 1-800-WX-BRIEF.”
The problem of hard-to-read codes and irrelevant information has been pointed out to the FAA for
more than 15 years. In 2012 it was even put into Public Law 112-153 (Pilot’s Bill of Rights) and
FAA was given one year to address. This incident makes it clear that there is much more work to
be done. This is a safety issue that calls for urgent action.
Finding 15 - Cockpit Voice Recorder: The Cockpit Voice Recorder (CVR), which would have
provided much more information on what happened, unfortunately, was overwritten during normal
operations. We are unable to say that the delay in reporting was deliberate and may never
understand all the reasons behind the several other procedural failures that allowed this incident to
get so close to catastrophe. The CVR would have provided a much better picture.
NTSB Aircraft Incident Report
72
As of this writing, the Board is considering a recommendation to extend CVR recording time to
25 hours so that valuable data are not lost. However, cockpit image recording investigators provide
another source of critical information, which will help to ensure that NTSB’s findings are
comprehensive, and recommendations are well targeted. An image recorder recommendation was
originally issued in 2000 (A-00-031).
Non-punitive response - Image recording technology currently exists in every other mode of public
transportation except commercial aviation. Some pilot groups are concerned about the right to
privacy and that the information gathered will be used punitively. Workplace right-to-privacy has
been extensively litigated but in safety-critical positions, it must take a backseat to human life.
Most importantly, the data, gathered routinely before an accident, will be invaluable in preventing
the next tragedy. This approach has been highly effective in FOQA. There may be some technical
challenges to address but the payoff in increased safety and accountability will be significant.
One of the strongest attributes of aviation is the concept of just culture or non-punitive corrective
action. When a mistake is made, most people put their best foot forward and attempt to minimize
a critical error, which is perfectly understandable. Some supervisors want to mete out sanctions to
“teach a lesson” or to make an example of the crew. Unless someone is habitually error prone and
they shouldn’t be in a safety-critical position, punitive response is completely ill-suited to critical
performance environments.
It’s almost a certainty this crew will never make such a mistake again and my hope is that they
will continue to fly to the normal end of their careers.
Everyone will gain much more from being introspective rather than judgmental on this incident.
We should reward all aviation personnel and celebrate when someone self-confesses a mistake and
learns from it. More importantly, the system learns from it and can take steps to eliminate event
precursors. This is a key factor in the decades-long decline in commercial aviation’s accident rate.
Fortunately, we’ll get another chance to put some fixes in place to make a highly improbable event
even less likely to reoccur.
Recommendation A-18-25 – Automatic Warning of Wrong surface landing: The
recommendation to require an automatic warning system for runway alignment for all aircraft is
redundant. All commercial aircraft and nearly all GA aircraft flying into Class B and C airports
are already equipped with runway alignment equipment – ILS, RNAV or FMS. Although Air
Canada requires their crews to use systems that would have prevented the misalignment, the crew
on the incident flight failed to program the system for unknown reasons. If the command bars and
raw data do not align by 500 feet above ground level – something is clearly wrong, and a go-
around is in order. This is basic checklist discipline – especially for night visual approaches.
In modern air carrier aircraft, the FMS autotunes the final approach aids so the pilots don’t have
to. In this incident, the Bridge Visual Approach was the only one in Air Canada’s FMS system that
did not have the autotune function. That certainly could have been misleading to a crew that was
used to always having the approach tuned for them. It was an unusual procedure; charts for such
procedures should highlight the need for verifying that electronic guidance is tuned. It might also
be mentioned in the dispatch package.
Recommendation A-18-26 – New Equipment or Software: The recommendation to require a
separate warning system in addition to the primary navigation system and be applicable to ALL
NTSB Aircraft Incident Report
73
aircraft flying into Class B and C airspace (especially light, non-turbine Part 91) is far too broad
and fails to put the focus on the heavier airplanes that are most likely to cause loss of life in a
ground surface collision.
I concur because safety takes preference but there should be reasonable risk management behind
recommendations. There was not enough data to fully support a dissenting view at the Board
meeting. An FAA risk assessment study was cited as the justification for this recommendation by
noting that 85% of taxiway or wrong runway landings occurred during Part 91 operations.
However, this study discussed before the Board meeting, noted in passing that GA incidents almost
always occurred in daylight visual conditions when collision was highly unlikely. FAA’s
assessment was that risk of a collision was “extremely improbable.”
My hope is that forthcoming software design will allow this recommendation to be implemented
without much added complexity of additional hardware added to cockpits. Perhaps it can be a part
of the Electronic Flight Bag (EFB).
Recommendation A-18-29 to Transport Canada on Fatigue Rules: Fatigue continues to be a
recurring factor in accidents and incidents. This captain had been awake for 19 hours. It’s estimated
that he awoke around 0800 Eastern time; the incident occurred at 0300 ET the following day.
While not technically on duty all that time, under Canadian regulations for reserve crew members,
he could have been available for duty for another nine hours. Adjusting circadian rhythm, even
with naps, is not a precise activity.
The captain’s statement as to why he did not make a timely incident report to dispatch after landing
was that “It was very late” and he “was tired.” The captain was too tired to make a phone call to
report the incident, but the rules required him to be able to fly a challenging night approach with
139 passengers and crew behind him. If we expect solid human performance where lives are at
stake, fatigue rules need to be based on human factors science and not on economic considerations.
Member Weener joined this statement.

NTSB Aircraft Incident Report
74
Member Weener filed the following concurring statement on October 4, 2018:
Member Earl F. Weener, Ph.D.
Concurring
As a longtime pilot and flight instructor, I understand that mistakes are inevitable for even the best
aviators. Thus, it is critical that safety systems are instilled with redundancy and multiple layers
which work effectively to mitigate, correct, or prevent these errors. I agree with findings and
conclusions but wonder if they go far enough. We have focused on what can be done in the future
to preserve the cockpit voice recorder. An opportunity to review a voice recording of events
leading to an incident is invaluable but does not serve the same function as an immediate evaluation
of a flight crew’s fitness for duty.
In this event a commercial aircraft filled with passengers came within feet of striking another
aircraft and causing a collision with several others on the ground. Over 1000 people were at
imminent risk of serious injury or death. The commercial operator had policies in place that
required the reporting of serious incidents and that would have removed the flight crew from
service immediately and until they could be evaluated for flight readiness. However, the subjective
observations of the crew as they flew over the aircraft on the ground and executed a go-around did
not prompt them to report anything to their operational control until the next day. Moreover, they
reportedly did not perceive the gravity of the situation, stating to NTSB investigator they did not
descend below 400ft prior to initiating a go-around. According to the crew, they did not realize
just how near they were to striking another aircraft.
In reality, the overflying crew may have been in a poor position to fully understand their proximity
to disaster because of their perspective, looking down at night, and their workload, as they executed
functions necessary to landing then undertook a go-around. And, although Air Canada procedures
required incidents be reported as soon as possible, the crew was apparently unclear on the meaning
of ASAP. They did not report the event to their Air Canada point of contact until the following
day. The bottom line is that reliance on self-reporting in this instance resulted in a flight crew that
only stopped flying that night because they had finished a shift. Had that not been the case, nothing
would have stopped them from flying additional trips immediately following this incident. In this
case, there turned out to be no medical issues or competency concerns with the crew. And, because
they happened to be at the end of shift, any fatigue issues were resolved. However, I am not
comforted because that despite a lack of immediate action, everyone made it home safely. I believe
more robust measures should be in place to intervene when a dangerous situation become apparent.
There was only one controller in the tower that night and his work load was significant. Yet, while
he was expected to continue his solo operation, he also had unique knowledge of the events that
had just occurred. It was the controller who called for the go-around, knew the Air Canada flight
almost landed on an active taxiway, reported the Air Canada crew was shaken, and stated that he
himself was other than calm after the event. When a pilot on the ground contacted the controller
to report the Air Canada flight had gone right over him, the controller replied that he had seen it
happen. Yet, the controller did not report the event in the system until the end of his shift. When
NTSB Aircraft Incident Report
75
he did so, it was only as a go-around and he chose not to mark the event as significant when
prompted by his reporting software.
The pilots on the taxiway that evening had perhaps the best perspective of what occurred, and one
even went so far as to switch on extra lighting to warn the approaching Air Canada flight away.
Yet, faced with the need to continue their own flights and without any requirement for immediate
reporting, the pilots on the ground took no immediate action prompting an intervention and
evaluation of the Air Canada crew.
I am left concerned that post-incident forensic analysis of a cockpit voice recorder, while vital,
cannot replace immediate, safety-focused interventions designed to take crews involved in near
miss situations out of service until they can be assessed as safe to continue. Whether it is industry,
the FAA, or airports that stand up a more effective “if you see something, say something” style
system regarding dangerous operational behavior, it is clear to me that the need exists.
Vice Chairman Landsberg and Member Dinh-Zarr joined this statement.
NTSB Aircraft Incident Report
76
5. Appendixes
Appendix A: Investigation
The National Transportation Safety Board (NTSB) was notified of this incident at
1630 eastern daylight time on July 9, 2017, by the Federal Aviation Administration (FAA). Two
NTSB investigators traveled to San Francisco International Airport (SFO) on July 15. Investigative
groups were formed in the areas of air traffic control and operations/human performance.
Specialists were assigned to perform the readout of the flight data recorder at the NTSB’s
laboratory in Washington, DC; conduct an aircraft performance study; and gather airport-related
information.
Parties to the investigation were the FAA, the National Air Traffic Controllers Association,
and Honeywell. In accordance with the provisions of Annex 13 to the Convention on International
Civil Aviation, the Bureau d’Enquêtes et d’Analyses pour la Sécurité de l’Aviation Civile (BEA),
the NTSB’s counterpart agency in France, participated in the investigation as the representative of
the state of design and manufacture, and Airbus participated in the investigation as a technical
advisor to the BEA. Also, the Transportation Safety Board of Canada (TSB), the NTSB’s
counterpart agency in Canada, participated in the investigation as the representative of the state of
the operator and registry, and Air Canada, the Air Canada Pilots Association, and
Transport Canada participated in the investigation as technical advisors to the TSB.
NTSB Aircraft Incident Report
77
Appendix B: Air Canada Postincident Actions
Air Canada reported, in e-mails to the NTSB dated April 17 through 20, 2018, that it took
the following actions after the incident:
• Developed a means for flight crews to use company tablets to highlight areas and make
notes on digital flight releases.
• Modified its procedures for the Flight Management System (FMS) Bridge approach to
runway 28R at SFO. The instruction to tune the instrument landing system frequency was
replaced with the instruction to use lateral and vertical navigation guidance to align an
airplane with the runway centerline on short final. Also, the FMS automatically sequences
the missed approach procedure when the thrust levers are advanced to the
takeoff/go-around detent.
• Began assessing the use of airplane systems to provide aural and visual alerts if an airplane
is not aligned with a runway. This capability is currently installed in company simulators
as part of an effort to determine the appropriate system settings to be used during normal
operations.
• Upgraded the Airbus A320 simulator and increased its fidelity so that the simulator
graphics could be set to replicate specific airports, including SFO.
• Implemented familiarization training for operations to and from SFO for all pilots during
recurrent training.
• Implemented a learning management system module for all airports on the FAA’s Special
Pilot-in-Command Qualification Airport list (including SFO), Air Canada restricted entry
airports, and unique airports within Air Canada’s system.
• Reiterated the requirement to back up all approaches with electronic means when available.
• Explained the meaning of “as soon as possible” (in revision 33 of the Flight Operations
Manual, which was issued in May 2018) for reporting aircraft accidents, incidents,
emergencies, and other safety events.
• Amended the arrival and approach briefing procedures (in revision 33 of the Flight
Operations Manual) to ensure that the approach and runway lighting and visual aids
expected for a runway are briefed.
NTSB Aircraft Incident Report
78
References
Bhattacherjee, Anol. 2001. “Understanding Information Systems Continuance: An
Expectation-Confirmation Model.” MIS Quarterly 25, no. 3 (September): 351-370.
Caldwell, John A. 1997. “Fatigue in the Aviation Environment: An Overview of the Causes and
Effects as well as Recommended Countermeasures.” Aviation, Space, and Environmental
Medicine 68 (10): 932-938.
Colman, Andrew M. 2006. Dictionary of Psychology. New York: Oxford University Press, 688.
FAA (Federal Aviation Administration). 2008. Aviation Instructor’s Handbook. FAA-H-8083-9A.
Washington, DC: US Department of Transportation, FAA Flight Standards Service.
———. 2017. “Fact Sheet—Commercial Aviation Safety Team.” Last modified December 27,
2017. https://www.faa.gov/news/fact_sheets/news_story.cfm?newsId=22455.
———. 2018a. “ADS-B, Airport Surface Surveillance Capability (ASSC).” Last modified
February 26, 2018. https://www.faa.gov/nextgen/programs/adsb/atc/assc/.
———. 2018b. “Wrong Surface Landing.” Published July 25, 2018. Video,
3:57. https://www.youtube.com/watch?v=5II-s_j35cI&feature=youtu.be.
Harrison, Y. and J.A. Horne. 1999. “One Night of Sleep Loss Impairs Innovative Thinking and
Flexible Decision Making.” Organizational Behavior and Human Decision Processes 78
(2): 128-145.
Khatwa, Ratan. 2004. “Flight Simulator Evaluation of Pilot Performance with the Runway
Awareness and Advisory System (RAAS).” The 23rd Digital Avionics Systems
Conference, Salt Lake City (October).
Marinelli, Rick. 1987. Development of a Visual Aid to Indicate Temporary Runway Closure. FAA
Technical Note DOT/FAA/CT-TN87/3, Atlantic City, New Jersey: FAA Technical Center
(January).
Nickerson, Raymond. 1998. “Confirmation Bias: A Ubiquitous Phenomenon in Many Guises.”
Review of General Psychology 2 (2): 175-220.
NTSB (National Transportation Safety Board). 1994. A Review of Flightcrew-Involved, Major
Accidents of U.S. Air Carriers, 1978 Through 1990. SS-94/01. Washington, DC: NTSB.
———. 2007. Attempted Takeoff From Wrong Runway, Comair Flight 5191, Bombardier
CL-600-2B19, Lexington, Kentucky, August 27, 2006. AAR-07/05. Washington, DC:
NTSB.
