Professional dissonance: A promising concept for clinical social work.
By: Melissa Floyd-Pickard
Taylor, M. F. (2007). Professional dissonance: A promising concept for clinical social work.
Smith College Studies in Social Work, 77 (1), 89-100.
This is an Author's Original Manuscript of an article whose final and definitive form, the
Version of Record, has been published in Smith College Studies in Social Work [2007]
[copyright Taylor & Francis], available online at:
http://www.tandfonline.com/10.1300/J497v77n01_05.
Abstract:
Social workers in mental health face a complex climate where they encounter value-laden
intervention choices daily. Examples of these choices may include deciding to initiate treatment
in spite of a client's wishes to the contrary, making a decision to break confidentiality, feeling
pressured to diagnose a client with a reimbursable condition despite a treatment philosophy that
may be to the contrary, or feeling the need to “pick and choose” therapy topics in light of severe
shortages in benefit coverage. These and other scenarios put social work clinicians at risk for
professional dissonance or what has been called a feeling of discomfort arising from the conflict
between professional values and expected or required job tasks. The current article explores
professional dissonance as a pertinent concept for social work in general, and mental health
social work in particular. The theory base of the concept is explored as well as its utility for
understanding burn-out in a deeper way.
burn-out | value dilemmas | ethical dilemmas | ethics | existentialism | social work | Keywords:
clinical social work | mental health
Article:
PROFESSIONAL DISSONANCE DEFINED
Professional dissonance is a new concept introduced here and is defined as a feeling of
discomfort arising from the conflict between professional values and job tasks. It has been
developed through the application of cognitive dissonance theory and existential theory to the
study of values and ethics and to the realities of practice climate in the mental health social work
arena. In this article, the author seeks to outline the philosophical background of professional
dissonance and its utility as a way of understanding the deeper dimensions of burn-out formental
health clinicians (see Figure 1).
In recent research findings (Taylor & Bentley, 2005), professional dissonance has been affirmed
as something seasoned mental health clinicians struggle with; however, the purpose of this article
is to explore the conceptual basis of professional dissonance. Accordingly, the research findings
will not be discussed in detail.
Social workers are regularly asked, and often required, to formulate practice decisions that both
protect society and maximize the rights of the individual–perhaps an impossible task. When the
two aims are incompatible, social workers find themselves in the position of making a practice
decision that may be unwanted and/or directly opposed by the consumer. An example of such a
decision would be requiring an actively psychotic but not currently dangerous consumer who is
handing out leaflets in the park to be hospitalized against his/her will. The decision to hospitalize
may conflict with the social worker’s value commitment to self-determination. In these and
many other situations, social workers have to deal with layers upon layers of competing values
(Loewenberg, Dolgoff, & Harrington, 2000). For example, they may have a personal
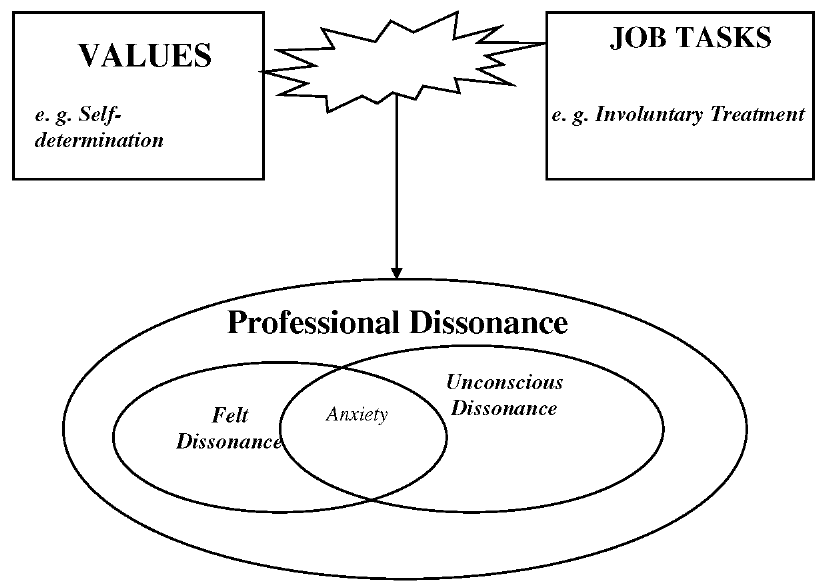
FIGURE 1. Schematic of Research Concepts
value about self-determination: “I believe in the importance of choice above all else”; a group
value: “I belong to X organization that opposes involuntary treatment”; a societal value: “I want
to feel safe when I take my kids to that park”; and a professional value: “Agency policy requires
me to intervene since I’m the case manager.” These value issues are further complicated by the
fact that the worker may encounter competing values on each one of the levels. For example, a
social worker, referring back to her/his professional values as exemplified in the NASW Code of
Ethics, encounters mixed direction: “I can intervene based on the NASW Code of Ethics, but the
Code also says I can restrict self-determination when it’s an imminent risk.” This exposition of
levels of values involved in daily social work decision making is but one example of the
potential complexity in intervention that faces mental health practitioners.
PHILOSOPHICAL BACKGROUND OF PROFESSIONAL DISSONANCE
The core ideas of existential theory have influenced psychology, literature, and sociology as well
as social work, and provide an important philosophical background in the conceptualization of
professional dissonance. Existential theory is important to professional dissonance because the
key existential issues of “authenticity” versus “bad faith,” and “ontological guilt” versus
“ontological anxiety,” speak to the current struggle in mental health practice to negotiate a social
work position that simultaneously protects a consumer’s rights (even to fail) and ensures the
practitioners’ ability to make professional, caring, and sometimes unpopular decisions about how
to intervene. Exploring the themes of existential philosophy also illuminates some reasons why
the perennial struggle inmental health, around what is right and what is wrong to do when
intervening in consumer’s lives, is so important. An existential philosophical background
additionally suggests why social workers need to feel good about the decisions they make and
what can happen when they do not.
Professional dissonance can accurately be classified as an existential problem in that it relates to
feelings which directly impact on our perception of ourselves as people, our feelings about the
kind of people and professionals we are, and our feelings about how we should live our lives and
fulfill our jobs. As Maddi (1996) points out, existential psychology, for all its diversity of
thought, emphasizes above all else the central tenets of being genuine, honest, and true, and of
“making decisions and shouldering responsibility for them” (p. 155). It is interesting to note that
these themes are the opposite characteristics of a state of depersonalization, a dimension of
unresolved burn-out (Pines & Maslach, 1978).
The dissonance and dissonance resolution processes are ones filled with confusion, angst and,
hopefully in the end, professional and personal growth. Pointing to a similar process, existential
philosophy affirms the opportunity for and necessity to form meaning out of suffering (Krill,
1996). Social work practice is filled with examples of consumers and families coming through
crises and illnesses with greater life understanding. Author and mental health consumer, Lori
Schiller (Schiller & Bennett, 1994) ends her biography as follows:
Looking over my life, I know now that I don’t want to go back. I want to go ahead . . . If
my life and my experiences can help other people find their ways out of darkness, I will
know that I have not wasted the great gift I have been given: the chance to begin life
again. (p. 270)
Similarly, when mental health practitioners confront feelings of angst, conflict, and frustration
before coming to the best practice decision they can, they are attempting to protect excellence in
practice.
While many aspects of existential theory have been helpful in developing the concept of
professional dissonance, the existential concepts of ontological guilt and ontological anxiety
have most influenced the conceptualization. In order to understand these ideas, the existential
concepts of being and being-in-the-world, authenticity, and bad faith are first presented and
briefly defined. An exposition of ontological guilt and ontological anxiety follows.
Being and Being-in-the-World. Existential philosophers place a great deal of emphasis on being.
Maddi (1996) points out that the German word for being (“daesin”) does not carry the static
connotation that “being” has in the English language. Instead, the word is more active and
actually means, “becoming.” In this way, the existential focus is on human potentiality. In order
to always be “becoming” and not have stagnated, the person must continue to act authentically
and avoid bad faith actions that delude and detract from the metamorphic process of becoming.
As it applies to mental health practitioners, the concept of being would, among other things,
connote continuing to develop as an excellent practitioner, working hard to lend individuality to
every practice situation, and having a dynamic, present orientation.
Authenticity versus Bad Faith Actions. Authenticity is often used as a synonym for genuineness.
Hepworth, Rooney, and Larsen (1997), in their widely used direct practice social work textbook,
define authenticity as “the sharing of self by relating in a natural, sincere, spontaneous, open and
genuine manner” (p. 120). They further describe the authentic social worker’s verbalizations as
congruent with their thoughts and feelings. In this way, they relate to consumers as real people,
expressing and taking responsibility for their feelings instead of denying them or blaming the
client for them. This focus on congruency between thoughts and feelings, and on assuming
responsibility for them whether or not they fit in with societal ideas of what is normal or good, is
closely related to the existential focus on authenticity. The existential hero, exemplified in texts
such as Camus’ (1946) The Stranger and Sartre’s (1947) The Age of Reason, embodies the ideal
of “authenticity” and is therefore often seen as abnormal or strange as s/he strives to realize
“being.” By acting in accordance with internal guidance, the existential hero avoids being
deluded by the trappings of normality and the conformity of society. In this way, bad faith
actions are guarded against and the individual continues her/his process of “becoming.”
Bad faith actions are the antithesis of authenticity. When an individual acts in a “bad faith” way,
s/he is acting against what his or her inner voice is directing. For example, a social worker who
internally supports an individual consumer’s stance not to take medication because the worker
believes that for this consumer the disadvantages outweigh the advantages, commits a bad faith
action when s/he pursues an inpatient commitment due to pressure from a supervisor or from the
consumer’s family. Similarly, a practitioner who upholds self-determination simply because s/he
doesn’t want to have to struggle with the paperwork involved in a commitment procedure, even
though the consumer needs to be hospitalized, commits a bad faith action as well. Individuals
who continually choose bad faith actions over authentic responses stop progressing as
“becoming” human beings. They may also stop taking responsibility (another key existential
concept) for their choices. In the examples above, the social workers may blame their choices on
society, on a difficult family, or even on the consumers themselves. But when the becoming
process halts, individuals become aware of feeling bad or being in psychological pain. According
to existential psychology, the individual feels bad due to the cumulative weight of ontological
guilt accumulated through repeated bad faith actions. Maddi (1996) suggests this is what Soren
Kierkegaard, one of the first existential philosophers, meant by the phrase “sickness unto death”
(p. 162), and what Thoreau was getting at when he said most people “lead lives of quiet
desperation” (p. 162).
Ontological Anxiety versus Ontological Guilt. In current research, dissonance is related to the
concept of anxiety, one that existential writers have long argued is misunderstood. Rollo May
(1983), a prominent existential author, wrote that the German word Freud and Kierkegaard,
among others, use for anxiety is “angst.” While it has no exact English equivalent, angst has
been translated as “dread” as well as “anxiety,” and captures the experience of being “torn,” or in
a dilemma. Accordingly, May points out that anxiety “always involves inner conflict” (p. 111).
Anxiety has a “becoming” quality in that it can lead to growth (Maddi, 1996). One has daily
choices either to continue becoming and face the resulting ontological anxiety, or to simply
choose comfort and stasis and therefore stagnate. Maddi describes ontological anxiety, or the
anxiety of becoming, quite eloquently:
Only when you have clearly seen the abyss and jumped into it with no assurance of
survival can you call yourself a human being. Then, if you survive, you shall be called a
hero, for you will have created your own life. (p. 162)
Quite simply, ontological anxiety is the price of living authentically. By contrast, choosing the
more comfortable, non-anxiety-provoking course of action will, in the short term, result in
feeling safer but in the long term lead to the more malignant state of “ontological guilt.”
Ontological anxiety, while uncomfortable, is more a pain of risk or a growing pain, while
ontological guilt is the pain of not accessing one’s potential, accompanied by the ache of regret
about “whatmight have been.” Series of bad faith actions result in heavy ontological guilt which
envelopes the individual in shame and regret, paralyzing their process of becoming.
One may well ask what all this abyss jumping has to do with intervention in mental health. But
existential psychology, with its focus on authenticity and responsibility, speaks directly to the
cost of bad faith actions (choosing not to jump). In this way, it answers the question of what
happens to social workers who consistently act in ways that conflict with their ideas about what
they should be doing, or as Margolin (1997) says, “who live in contradiction.” It also changes the
negative cast usually given to anxiety, and encompasses anxiety as a potential growing
experience. In this way, existential psychology balances the prevailing view of anxiety as burn-
out or pathological by casting it as a growing pain. The recasting is compatible with the concept
of professional dissonance, which combines the view of anxiety as problematic (as seen in
cognitive psychology and ego psychology) with the idea of anxiety as a possible vehicle toward
practice excellence.
PROFESSIONAL DISSONANCE AND BURN-OUT
Burn-Out, the “syndrome of physical and emotional exhaustion, involving the development of
negative self-concept, negative job attitudes, and a loss of concern and feeling for clients” (Pines
& Maslach, 1978, p. 224), has been called an occupational hazard for human service providers
(Gomez &Michaelis, 1995). Additionally, social workers in mental health are more likely to
experience burn-out and have decreased job satisfaction as comparedwith social workers in other
areas (Acker,1999). The three-dimensional construct of burn-out includes emotional exhaustion,
depersonalization, and feelings of reduced personal accomplishment (Enzmann, Schaufeli,
Janssen, & Roseman, 1998). As a concept, professional dissonance seeks to add a new element
to the discussion around burn-out and job satisfaction by exploring the ways social workers feel
torn or ambivalent about the ways their values and work interventions coexist. For example, a
practitioner may have worked tirelessly to help a consumer attain disability benefits that the
practitioner feels are desperately needed. The consumer, upon getting the hard-won benefits,
may decide that s/he really should work, despite not having been able to keep a job for more than
a few weeks in the past. In this example, the client’s wishes and right to self-determine must be
weighed against the practitioner’s view of the situation in making a decision about how to
intervene. In short, professional dissonance relates to the burn-out literature in that it attempts to
understand the inner lives of social workers and how their inner thoughts and outer actions may
contribute to burn-out.
PROFESSIONAL DISSONANCE AND COGNITIVE DISSONANCE THEORY
The theory of professional dissonance was conceptualized by Leon Festinger and other cognitive
theorists. Festinger (1962) developed cognitive dissonance theory in the 1960s as a “consistency
theory,” so designated because it emphasizes the premise that humans desire congruence in their
thinking and will act to reduce inconsistency among thoughts, and between thoughts and
behaviors. He defines cognitive dissonance as “the existence of nonfitting relations among
cognitions” (p. 3). In other words, a person who has two cognitions that are inconsistent,
experiences dissonance–a negative drive state similar to hunger or thirst (Aronson, 1997).
Festinger goes on to describe the reduction of dissonance as a basic process among humans.
More recently, Aronson (1997) expanded Festinger’s more “cerebral” brand of cognitive
dissonance by emphasizing the role behavior plays in causing dissonance. Aronson
conceptualizes dissonance as strongest when a cognition related to self-concept conflicts with a
cognition about behavior. In other words, dissonance is strong when an action contradicts a
belief about the self. This type of cognitive dissonance–the conflict between behavior and self-
concept–is seen as giving rise to professional dissonance. As it applies to social workers,
professional dissonance can occur when an individual’s identification with her/his professional
values conflicts with certain expected or required job tasks.
The issue of insight or perception in the conceptualization of professional dissonance is very
important. A social worker who has experienced and successfully resolved her/his dissonance,
whether positively or negatively, may not be aware of the process s/he went through to come
through the dissonant situation. On the other hand, another social worker may be very aware of
the parts of her/his job situation that create discomfort by placing her/him in a value-dissonant
position. For this reason, the dimension of felt value/job conflict is important in understanding
professional dissonance. It joins the other dimensions, unconscious dissonance and felt anxiety,
in framing the experience of professional dissonance (see Figure 1). It is simply defined as the
actual, felt, or reported discrepancy between a job intervention, such as placing a consumer in the
hospital against her/his wishes, and a professional value such as self-determination.
Festinger (1962) outlines three types of relationships among cognitions: irrelevance, consonance,
and dissonance. In an irrelevant relationship, the two cognitions have no relationship (“That
consumer is creative and energetic,” “I’m out of Post-It notes”). When cognitions are consonant,
the cognitions are consistent and complement one another (“That consumer is creative and
energetic,” “I really like that consumer”). In the final relationship, the two cognitions conflict
with one another (“That consumer is creative and energetic,” “The consumer is becoming manic
and needs to be hospitalized”). Dissonant cognitions result in discomfort accompanied by a
desire to make the cognitions more consonant, and thereby alleviate the discomfort (“It’s ok to
be high energy but she’s going too far,” “If I don’t act now she may get worse”).
In understanding the way professional dissonance applies to clinical practice, it is important to
explore how clinicians employ dissonance resolution strategies in attempting to alleviate their
discomfort (“I’m acting in her best interests, that’s my job,” “She’s been hospitalized a lot, one
more time is not going to make that much of an impact”). In this example, the social worker who
feels dissonant about having to hospitalize her/his “favorite” consumer, first attempts to
rationalize the intervention and then minimizes the impact of the intervention on the consumer.
The goal is to alleviate the social worker’s dissonance. In summarizing cognitive dissonance as a
theory, Harmon-Jones and Mills (1999) cite four ways in which dissonance can be reduced: (1)
by removing the dissonant cognition: “I had no choice”; (2) by adding new consonant cognitions:
“I’m helping her”; (3) by reducing the importance of dissonant cognitions: “She really doesn’t
mind being in the hospital”; and, (4) by increasing the importance of consonant cognitions: “Her
safety is the most important thing.” This last strategy mirrors the process of ranking values by
importance in individual situations that Loewenberg, Dolgoff, and Harrington (2000) have
described.
An individual clinician’s insight into his or her own dissonance reduction processes may wax
and wane, in much the way a person may unconsciously use a defense to manage anxiety without
being aware of what s/he is doing. Even if the person is aware, once experienced dissonance has
been reduced or resolved, s/he is comfortable again and has a stake in remaining comfortable
instead of rehashing the reasons for the initial dissonance. This is important in understanding
professional dissonance as a supervisory issue, because the clinical supervisor’s role may be to
stimulate dissonant discussions that raise anxiety in an effort to illuminate constructive
dissonance reduction. This again underlines existential theory’s emphasis on anxiety as growing
pains, versus society’s current stance that anxiety is pathological.
PROFESSIONAL DISSONANCE’S IMPORTANCE TO SOCIAL WORK PRACTICE
The concept of professional dissonance is significant to clinical social work practice for several
reasons. First, it draws attention to the phenomena as it affects clinical social work theory and
practice, and underlines the need for future inquiry into practice-based issues in mental health.
Second, it illuminates the complexities and ramifications of social work practice decision making
in cases that present value collisions (Frankl, 1988). In this way, it makes social work values,
particularly the value of self-determination, an area of future inquiry, and an essential topic for
practice-based research. Finally, the study of professional dissonance has implications for
practitioners’ relationships with consumers in mental health practice, and for the makers of
mental health policy.
Conceptualizing professional dissonance adds another dimension to research about burn-out and
the protection of job satisfaction. The ways in which social workers operationalize social work
values and use them to guide their practice needs to be studied further (Rothman, Smith,
Nakashima, Paterson, &Mustin, 1996) as does the way practitioners rank order values by
importance, depending on practice situations (Loewenberg, Dolgoff, & Harrington, 2000).
Creative, effective strategies for supporting practitioners in negotiating difficult practice
decisions need to be prioritized in order to insure longevity, despite contradictions in mission and
values and actual practice life (Margolin, 1997). Professional dissonance emphasizes the
imperative nature of research that aims to support practitioners in the decisions they make around
practice interventions with mental health consumers.
Social work in today’s practice environments is complex. Accordingly, it is essential that the
profession support an ongoing dialog and facilitate an engaging climate in which
multidimensional issues that lend clarity to value dilemmas in practice can be explored. Social
work values need to be concretized for daily practice, so they take on real-life meaning and
benefit both consumers and social workers. Focusing attention on values and value conflicts
protects the mission of social work and vitalizes the Code of Ethics with living examples of its
value and domain in daily clinical practice. Consistent support and protection of career
satisfaction ensures individual social worker’s longevity in the profession, improves consumers’
quality of life, and facilitates excellence in the profession’s continued partnership with persons
who have mental illness.
Social workers need to feel safe in their organizations if they are to continually analyze ongoing
practice decisions. Professional dissonance need not have negative effects if room is made in
professional organizations and in agencies for ongoing dialogue and value clarification. In this
way, the existential focus on anxiety as a possible vehicle for growth is applied to experiences of
professional dissonance in day-to-day practice. By supporting social workers in deliberating
about practice issues, we foster a healthy tension that may well lead to more innovative practice
and policy interventions.
REFERENCES
Acker, G. M. (1999). The impact of clients’ mental illness on social workers’ job satisfaction and
burnout. Health and Social Work, 24(2), 112-120.
Aronson, E. (1997). A theory of cognitive dissonance. American Journal of Psychology, 110(1),
127-137.
Camus, A. (1946). The stranger. New York, NY: Vintage Books.
Enzmann, D., Schaufeli, W. B., Janssen, P., & Rozeman, A. (1998). Dimensionality and validity
of the Burnout Measure. Journal of Occupational and Organizational Psychology, 71(4), 331-33.
Festinger, L. (1962). A theory of cognitive dissonance. Stanford, CA: Stanford University Press.
Frankl,V. E. (1988). The will to meaning: Foundations and applications of Logotherapy
(Expanded edition). New York, NY: Penguin Books.
Gomez, J. S. & Michaelis, R. C. (1995) An assessment of burnout in human service providers.
The Journal of Rehabilitation, 61(1), 23-27.
Harmon-Jones, E. & Mills, J. (1999). An introduction to cognitive dissonance theory and an
overview of current perspectives on the theory. In E. Harmon-Jones & J. Mills (Eds.), Cognitive
dissonance: Progress on a pivotal theory in social psychology (pp. 3-24). Washington, DC:
American Psychological Association.
Hepworth, D. H., Rooney, R. H., & Larsen, J. (1997). Direct social work practice (5
th
edition).
California: Brooks/Cole.
Krill, D. F. (1996). Existential social work. In Francis J. Turner (Ed.), Social work treatment (pp.
250-281). New York, NY: The Free Press.
Loewenberg, F. M., Dolgoff, R., & Harrington (2000). Ethical decisions for social work practice
(6th ed.). Itasca, IL: F. E. Peacock.
Maddi, S. R. (1996). Personality theories: A comparative analysis (6th edition). Brooks/Cole
Publishing.
Margolin, L. (1997) Under the cover of kindness: The invention of social work. Charlottesville,
VA: The University Press of Virginia.
May, R. (1983). The discovery of being. New York, NY: W.W. Norton & Company.
Pines, A. & Maslach, C. (1978). Characteristics of staff burnout in mental health settings.
Hospital and Community Psychiatry, 29, 223-233.
Rothman, J., Smith, W., Nakashima, J., Paterson, M., & Mustin, J. (1996). Client self
determination and professional intervention: striking a balance. Social Work, 41, 396-405.
Sartre, J. (1947). The age of reason. New York, NY: Albert Knopf.
Schiller, L. & Bennett, A. (1994). The quiet room: A journey out of the torment of madness.
New York, NY: Warner Books.
Taylor, M. F. & Bentley, K. J. (2005). Professional dissonance: Colliding values and job tasks in
mental health practice. Community Mental Health Journal, 41(4), 469-480.
